

Systematic Review of Beta-Lactam vs. Beta-Lactam plus Aminoglycoside Combination Therapy in Neutropenic Cancer Patients
- PMID: 38792012
- PMCID: PMC11487387
- DOI: 10.3390/cancers16101934
Systematic Review of Beta-Lactam vs. Beta-Lactam plus Aminoglycoside Combination Therapy in Neutropenic Cancer Patients
Erratum in
-
Correction: Ishikawa et al. Systematic Review of Beta-Lactam vs. Beta-Lactam plus Aminoglycoside Combination Therapy in Neutropenic Cancer Patients. Cancers 2024, 16, 1934.Cancers (Basel). 2024 Jun 19;16(12):2274. doi: 10.3390/cancers16122274. Cancers (Basel). 2024. PMID: 38927994 Free PMC article.
Abstract
We performed a systematic review of studies that compared beta-lactams vs. beta-lactams plus aminoglycosides for the treatment of febrile neutropenia in cancer patients.
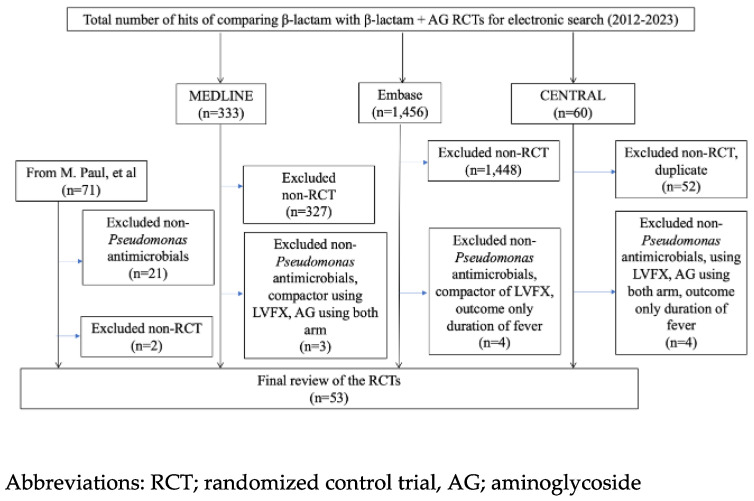
Method: We searched CENTRAL, MEDLINE, and Embase for studies published up to October 2023, and randomized controlled trials (RCTs) that compared anti-Pseudomonas aeruginosa beta-lactam monotherapy with any combination of an anti-Pseudomonas aeruginosa beta-lactam and an aminoglycoside were included.
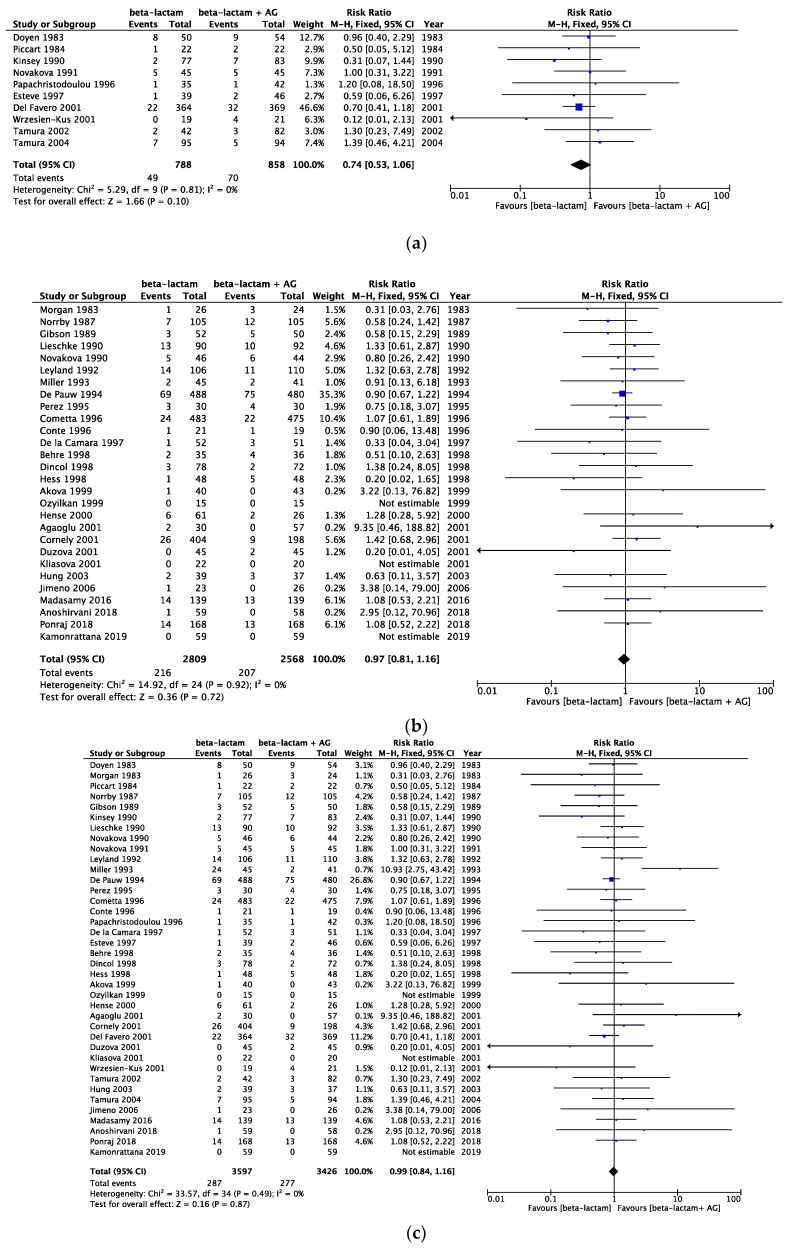
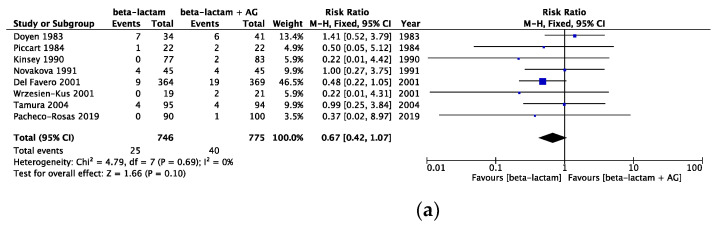
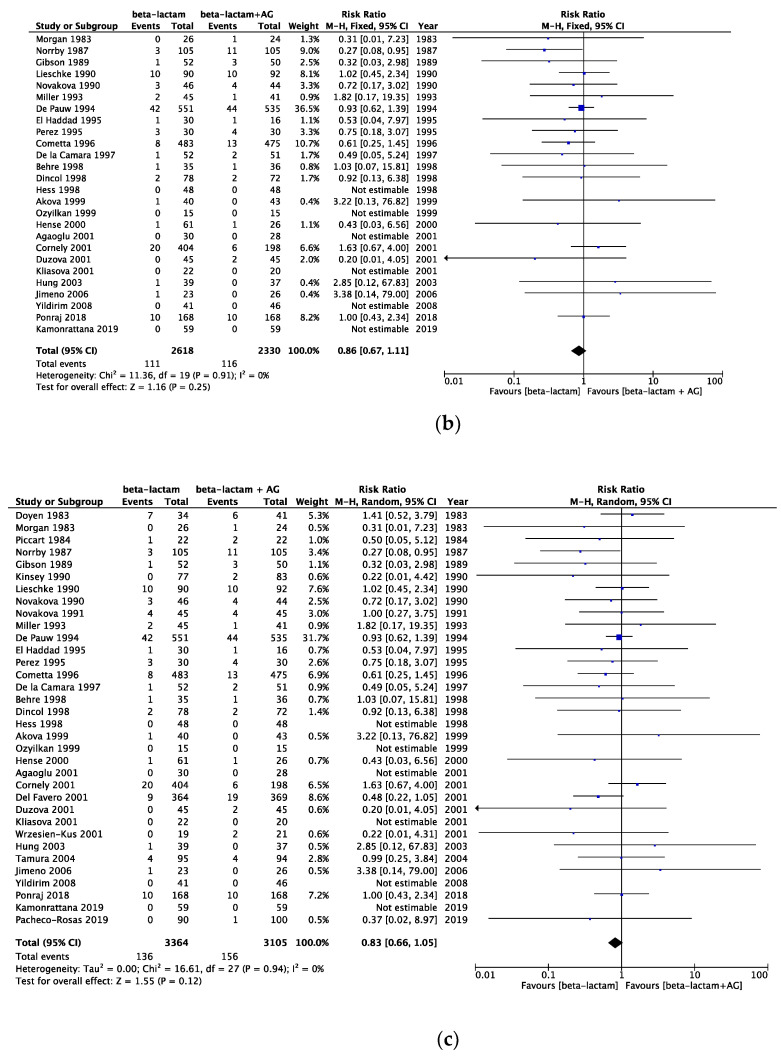
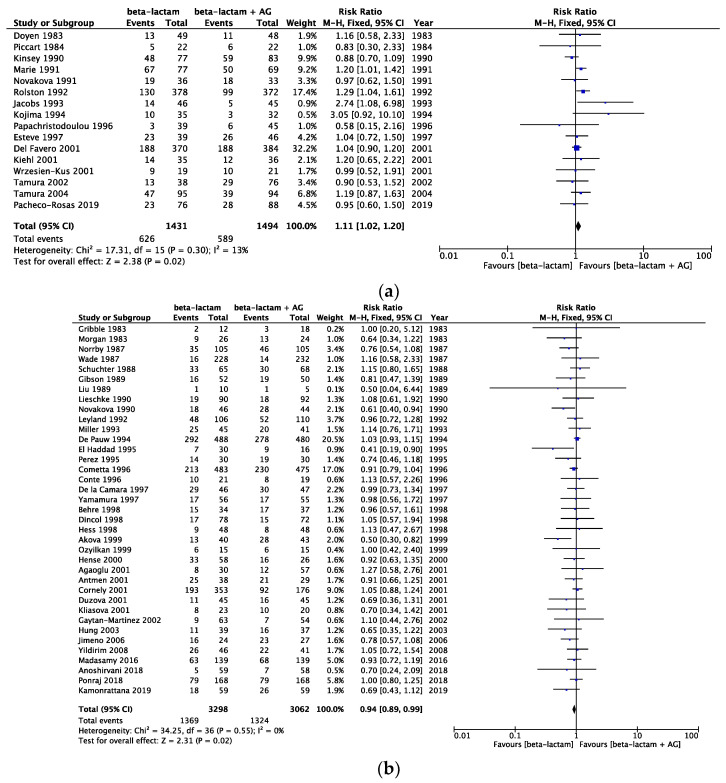
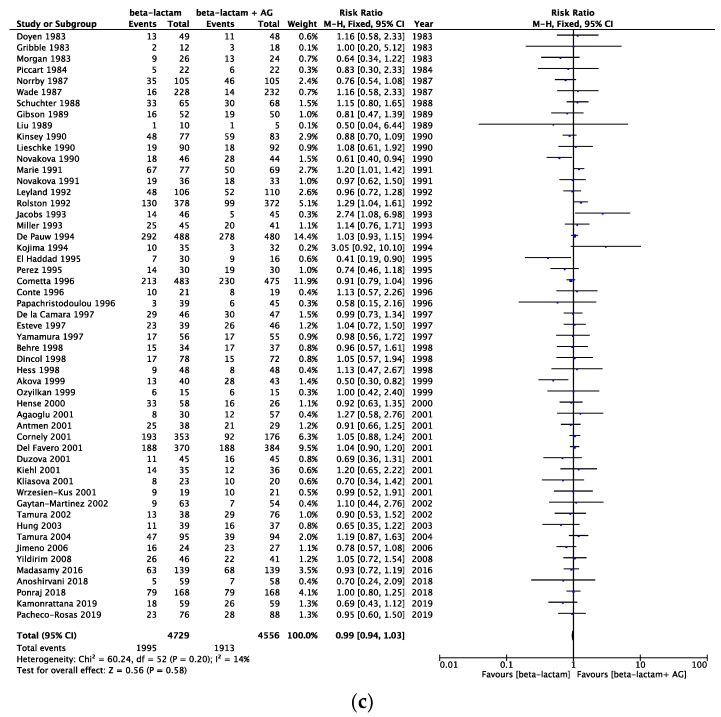
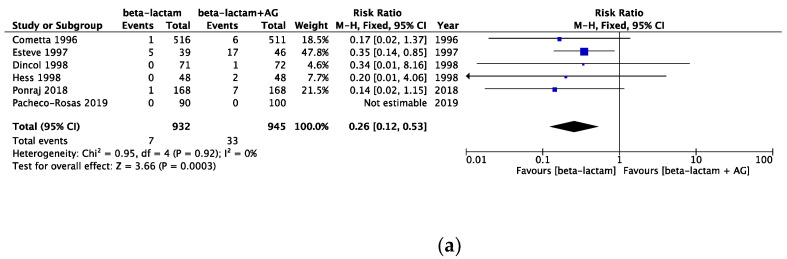
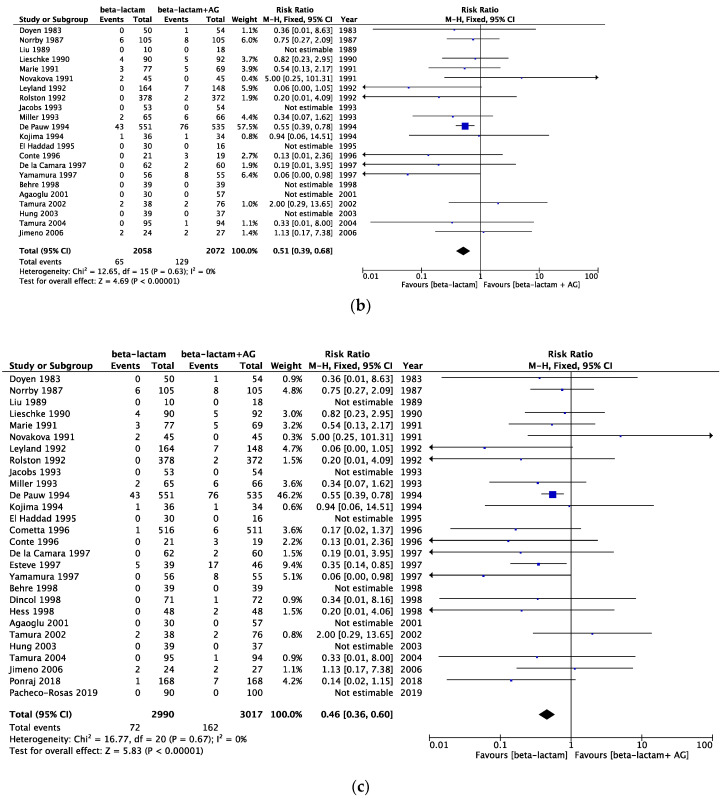
Result: The all-cause mortality rate of combination therapy showed no significant differences compared with that of monotherapy (RR 0.99, 95% CI 0.84 to 1.16, high certainty of evidence). Infection-related mortality rates showed that combination therapy had a small positive impact compared with the intervention with monotherapy (RR 0.83, 95% CI 0.66 to 1.05, high certainty of evidence). Regarding treatment failure, combination therapy showed no significant differences compared with monotherapy (RR 0.99, 95% CI 0.94 to 1.03, moderate certainty of evidence). In the sensitivity analysis, the treatment failure data published between 2010 and 2019 showed better outcomes in the same beta-lactam group (RR 1.10 [95% CI, 1.01-1.19]). Renal failure was more frequent with combination therapy of any daily dosing regimen (RR 0.46, 95% CI 0.36 to 0.60, high certainty of evidence).
Conclusion: We found combining aminoglycosides with a narrow-spectrum beta-lactam did not spare the use of broad-spectrum antibiotics. Few studies included antibiotic-resistant bacteria and a detailed investigation of aminoglycoside serum levels, and studies that combined the same beta-lactams showed only a minimal impact with the combination therapy. In the future, studies that include the profile of antibiotic-resistant bacteria and the monitoring of serum aminoglycoside levels will be required.
Keywords: beta-lactam plus aminoglycoside; cancer patient; combination therapy; febrile neutropenia.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
β-lactam antibiotic versus combined β-lactam antibiotics and single daily dosing regimens of aminoglycosides for treating serious infections: A meta-analysis.Int J Antimicrob Agents. 2020 Mar;55(3):105839. doi: 10.1016/j.ijantimicag.2019.10.020. Epub 2019 Nov 5. Int J Antimicrob Agents. 2020. PMID: 31704215
-
Ciprofloxacin vs an aminoglycoside in combination with a beta-lactam for the treatment of febrile neutropenia: a meta-analysis of randomized controlled trials.Mayo Clin Proc. 2005 Sep;80(9):1146-56. doi: 10.4065/80.9.1146. Mayo Clin Proc. 2005. PMID: 16178494
-
Effect of Using Aminoglycosides for Treatment of Sepsis [Internet].Oslo, Norway: Knowledge Centre for the Health Services at The Norwegian Institute of Public Health (NIPH); 2015 Feb. Report from Norwegian Knowledge Centre for the Health Services (NOKC) No. 3-2015. Oslo, Norway: Knowledge Centre for the Health Services at The Norwegian Institute of Public Health (NIPH); 2015 Feb. Report from Norwegian Knowledge Centre for the Health Services (NOKC) No. 3-2015. PMID: 28510405 Free Books & Documents. Review.
-
Comparative review of combination therapy: two beta-lactams versus beta-lactam plus aminoglycoside.Am J Med. 1986 Jun 30;80(6B):29-38. doi: 10.1016/0002-9343(86)90476-6. Am J Med. 1986. PMID: 3524218 Review.
-
Effect of aminoglycoside and beta-lactam combination therapy versus beta-lactam monotherapy on the emergence of antimicrobial resistance: a meta-analysis of randomized, controlled trials.Clin Infect Dis. 2005 Jul 15;41(2):149-58. doi: 10.1086/430912. Epub 2005 May 31. Clin Infect Dis. 2005. PMID: 15983909
Cited by
-
Correction: Ishikawa et al. Systematic Review of Beta-Lactam vs. Beta-Lactam plus Aminoglycoside Combination Therapy in Neutropenic Cancer Patients. Cancers 2024, 16, 1934.Cancers (Basel). 2024 Jun 19;16(12):2274. doi: 10.3390/cancers16122274. Cancers (Basel). 2024. PMID: 38927994 Free PMC article.
References
-
- Freifeld A.G., Bow E.J., Sepkowitz K.A., Boeckh M.J., Ito J.I., Mullen C.A., Raad I.I., Rolston K.V., Young J.A., Wingard J.R., et al. Clinical practice guideline for the use of antimicrobial agents in neutropenic patients with cancer: 2010 update by the infectious diseases society of america. Clin. Infect. Dis. 2011;52:e56–e93. doi: 10.1093/cid/cir073. - DOI - PubMed
-
- Averbuch D., Orasch C., Cordonnier C., Livermore D.M., Mikulska M., Viscoli C., Gyssens I.C., Kern W.V., Klyasova G., Marchetti O., et al. European guidelines for empirical antibacterial therapy for febrile neutropenic patients in the era of growing resistance: Summary of the 2011 4th European Conference on Infections in Leukemia. Haematologica. 2013;98:1826–1835. doi: 10.3324/haematol.2013.091025. - DOI - PMC - PubMed
-
- Leibovici L., Paul M., Poznanski O., Drucker M., Samra Z., Konigsberger H., Pitlik S.D. Monotherapy versus beta-lactam-aminoglycoside combination treatment for gram-negative bacteremia: A prospective, observational study. Antimicrob. Agents Chemother. 1997;41:1127–1133. doi: 10.1128/AAC.41.5.1127. - DOI - PMC - PubMed
-
- Paul M., Dickstein Y., Schlesinger A., Grozinsky-Glasberg S., Soares-Weiser K., Leibovici L. Beta-lactam versus beta-lactam-aminoglycoside combination therapy in cancer patients with neutropenia. Cochrane Database Syst. Rev. 2013;2013:CD003038. doi: 10.1002/14651858.CD003038.pub2. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
