

Management of Neonatal Hepatic Hemangiomas: A Single-Center Experience Focused on Challenging Cases
- PMID: 38792380
- PMCID: PMC11122465
- DOI: 10.3390/jcm13102839
Management of Neonatal Hepatic Hemangiomas: A Single-Center Experience Focused on Challenging Cases
Abstract
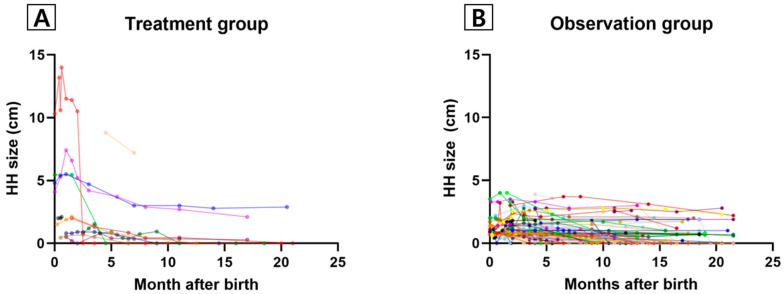
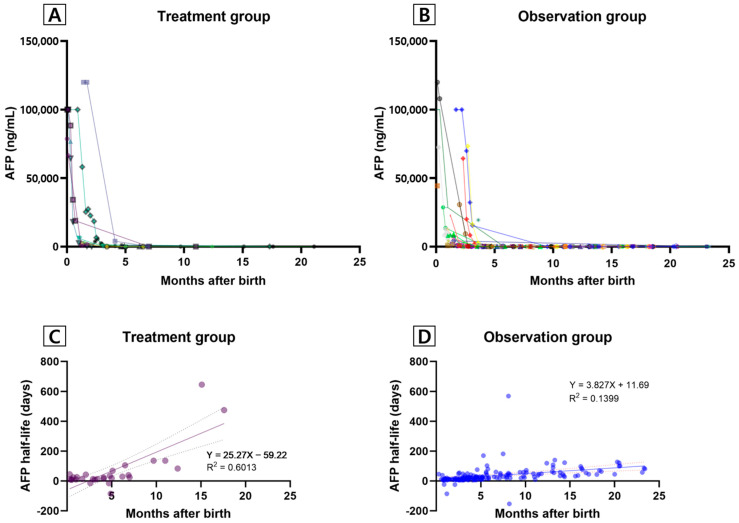
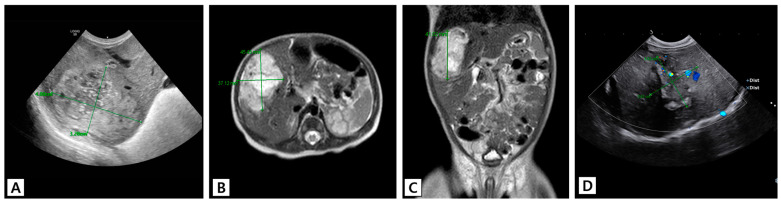
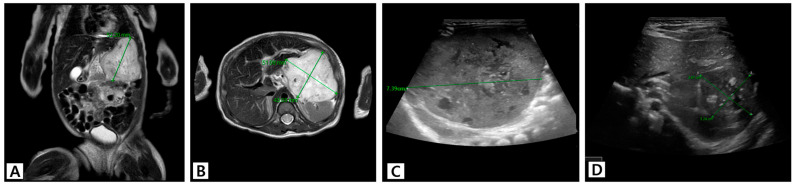
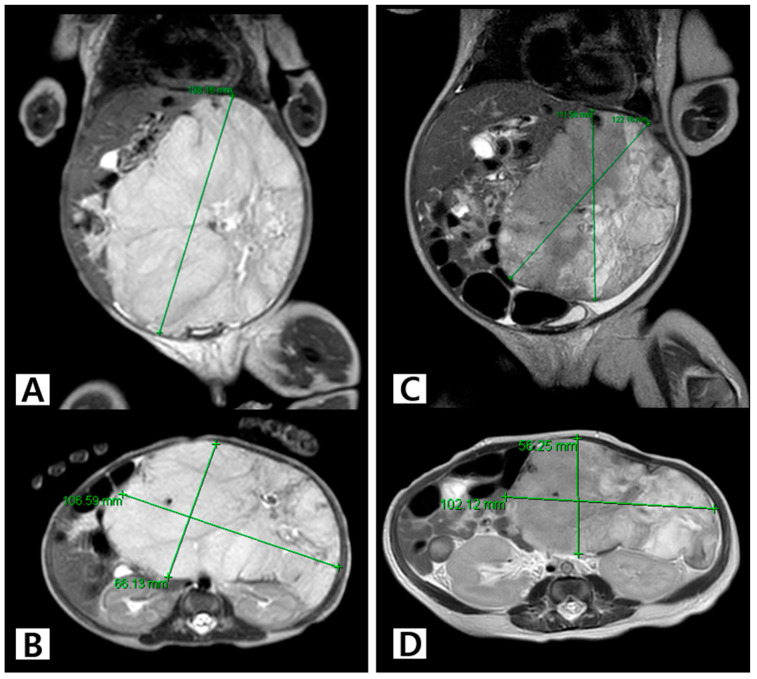
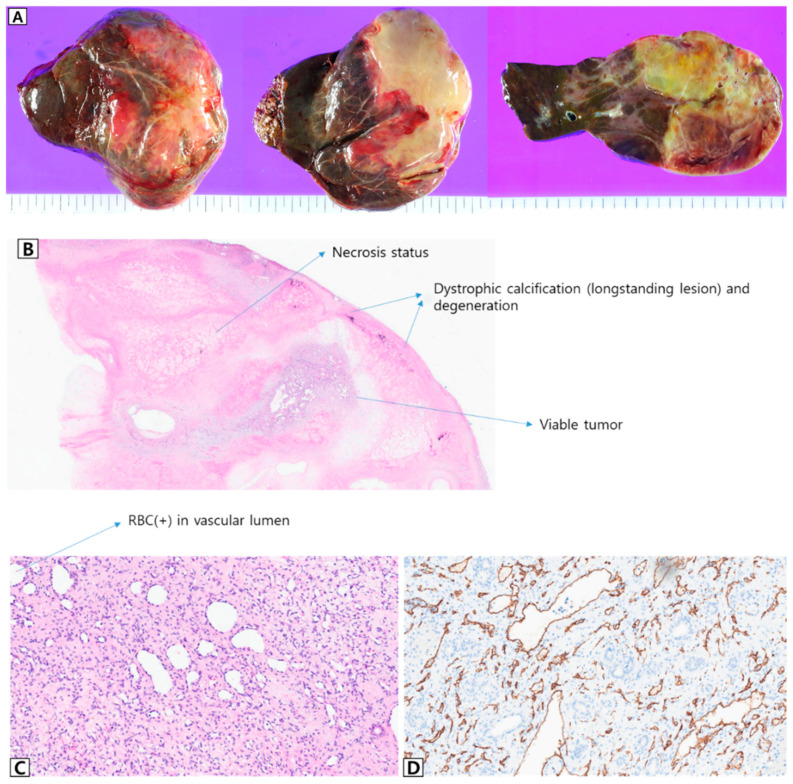
Background: Management of hepatic hemangioma (HH) in infancy ranges from close monitoring to surgical resection. We analyzed the clinical characteristics and outcomes of HH according to its treatment options, with particular focus on challenging cases. Methods: Data of patients diagnosed with HHs in their first year of life and followed up for at least 1 year were retrospectively reviewed and divided into treatment and observation groups. Serial imaging results, serum alpha-fetoprotein (AFP) levels, medications, and clinical outcomes were compared. The detailed clinical progress in the treatment group was reviewed separately. Results: A total of 87 patients (75 in the observation group and 12 in the treatment group) were included. The median HH size at the initial diagnosis and the maximum size were significantly larger in the treatment group than the observation group (2.2 [0.5-10.3] cm vs. 1.0 [0.4-4.0] cm and 2.1 [0.7-13.2] vs. 1.1 [0.4-4.0], respectively; all p < 0.05]. The median initial and last serum AFP levels were significantly higher in the treatment group than in the observation group (76,818.7 vs. 627.2 and 98.4 vs. 8.7, respectively; all p < 0.05). Serum AFP levels in both groups rapidly declined during the first 3 months of life and were almost undetectable after 6 months. Among the challenging cases, a large (14 × 10 × 6.5 cm sized) focal HH was successfully treated using stepwise medical-to-surgical treatment. Conclusions: Patients with large HH and mild symptoms can be treated using stepwise pharmacotherapy. More aggressive surgical treatment of tumors unresponsive to initial pharmacotherapy may help shorten the treatment period and improve outcomes.
Keywords: alpha-fetoprotein; hepatic hemangioma; propranolol; sirolimus; treatment outcome.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
A Retrospective Analysis of Clinical Characteristics, Treatment Modalities and Outcome of the Patients With Infantile Hepatic Hemangiomas: Single-center Experience From Turkey.J Pediatr Hematol Oncol. 2023 Mar 1;45(2):e259-e265. doi: 10.1097/MPH.0000000000002472. Epub 2022 May 5. J Pediatr Hematol Oncol. 2023. PMID: 35537066
-
Fetal and neonatal hepatic tumors.J Pediatr Surg. 2007 Nov;42(11):1797-803. doi: 10.1016/j.jpedsurg.2007.07.047. J Pediatr Surg. 2007. PMID: 18022426 Review.
-
Treatment of Symptomatic Focal Hepatic Hemangioma with Propranolol in Neonates: Is It Efficient?Pediatr Gastroenterol Hepatol Nutr. 2023 Jan;26(1):70-77. doi: 10.5223/pghn.2023.26.1.70. Epub 2023 Jan 10. Pediatr Gastroenterol Hepatol Nutr. 2023. PMID: 36816438 Free PMC article.
-
Historical and Contemporary Management of Infantile Hepatic Hemangioma: A 30-year Single-center Experience.Ann Surg. 2022 Jan 1;275(1):e250-e255. doi: 10.1097/SLA.0000000000003881. Ann Surg. 2022. PMID: 33064395
-
Hepatic hemangioma -review-.J Med Life. 2015;8 Spec Issue(Spec Issue):4-11. J Med Life. 2015. PMID: 26361504 Free PMC article. Review.
Cited by
-
A report of 12 cases of congenital hepatic hemangioma and literature review.Front Pediatr. 2025 Apr 28;13:1453019. doi: 10.3389/fped.2025.1453019. eCollection 2025. Front Pediatr. 2025. PMID: 40356783 Free PMC article.
-
Editorial: Recent advances in childhood vascular tumors.Front Oncol. 2024 Jul 25;14:1465155. doi: 10.3389/fonc.2024.1465155. eCollection 2024. Front Oncol. 2024. PMID: 39119090 Free PMC article. No abstract available.
References
-
- Al I.O., Demirağ B., Erdem M., Genç S., Karapinar T.H. A Retrospective Analysis of Clinical Characteristics, Treatment Modalities and Outcome of the Patients with Infantile Hepatic Hemangiomas: Single-center Experience from Turkey. J. Pediatr. Hematol. Oncol. 2023;45:e259–e265. - PubMed
-
- Triana P., Rodríguez-Laguna L., Giacaman A., Salinas-Sanz J.A., Martín-Santiago A., López-Santamaría M., Palacios E., Beato M.J., Martinez-González V., López-Gutierrez J.C. Congenital hepatic hemangiomas: Clinical, histologic, and genetic correlation. J. Pediatr. Surg. 2020;55:2170–2176. doi: 10.1016/j.jpedsurg.2020.02.008. - DOI - PubMed
LinkOut - more resources
Full Text Sources
