

Effects of Postoperative Gum Chewing on Recovery of Gastrointestinal Function Following Laparoscopic Gynecologic Surgery: Systematic Review and Meta-Analysis of Prospective Studies
- PMID: 38792393
- PMCID: PMC11121968
- DOI: 10.3390/jcm13102851
Effects of Postoperative Gum Chewing on Recovery of Gastrointestinal Function Following Laparoscopic Gynecologic Surgery: Systematic Review and Meta-Analysis of Prospective Studies
Erratum in
-
Correction: Tuscharoenporn et al. Effects of Postoperative Gum Chewing on Recovery of Gastrointestinal Function Following Laparoscopic Gynecologic Surgery: Systematic Review and Meta-Analysis of Prospective Studies. J. Clin. Med. 2024, 13, 2851.J Clin Med. 2025 Mar 26;14(7):2252. doi: 10.3390/jcm14072252. J Clin Med. 2025. PMID: 40217985 Free PMC article.
Abstract
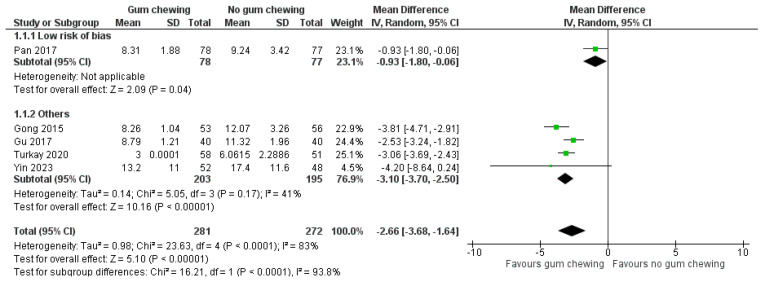
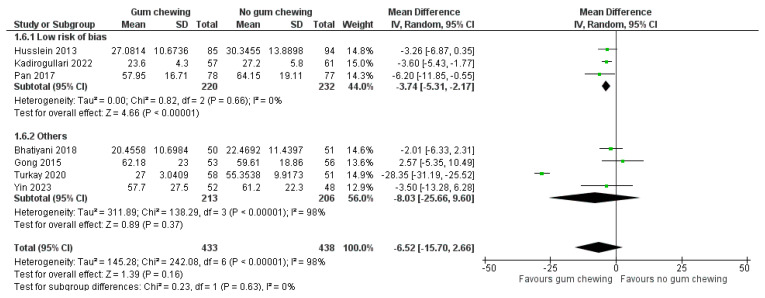
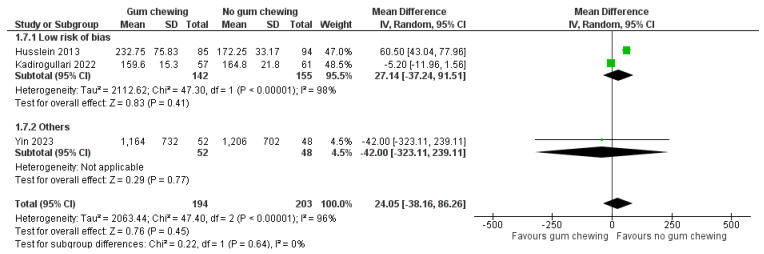
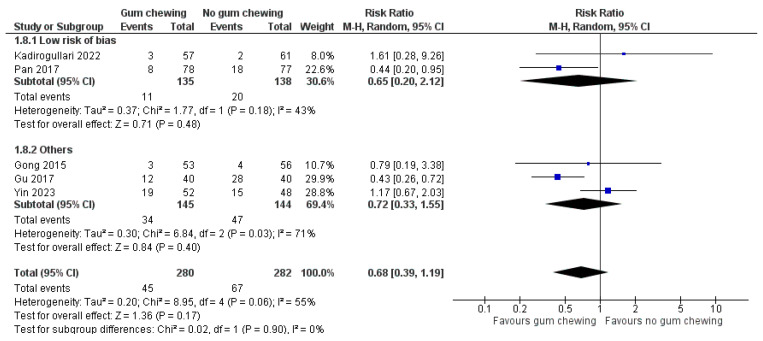
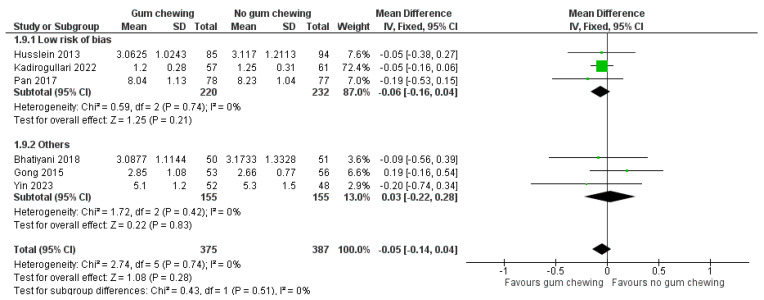
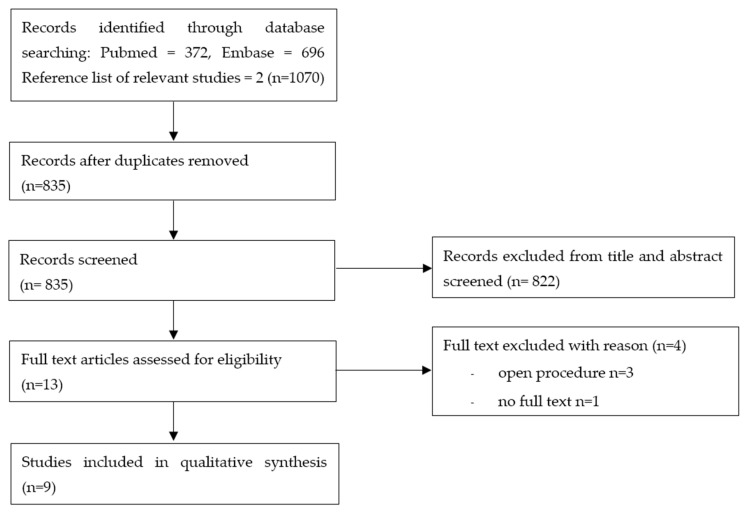
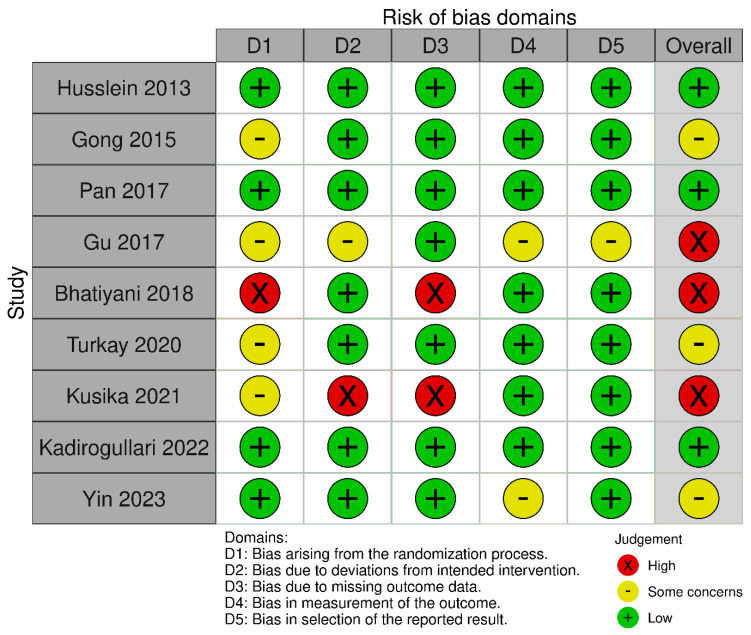
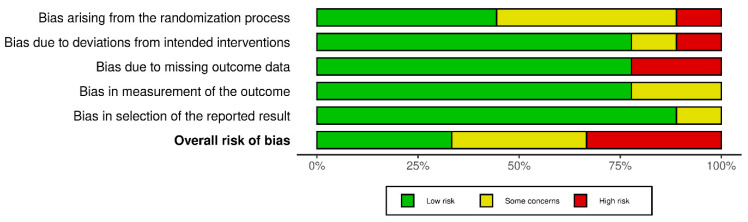
Background: Chewing gum, considered a form of sham feeding, has been shown to improve intestinal motor and secretory function in various types of abdominal surgery. We conducted this systematic review to evaluate the effects of postoperative gum chewing on the recovery of gastrointestinal function after laparoscopic gynecologic surgery. Methods: We performed a comprehensive literature review of all prospective clinical trials in PubMed, Embase, and a reference list of relevant studies from the inception to 11 March 2024, comparing postoperative gum chewing versus no gum chewing following laparoscopic gynecologic surgery regardless of indications and setting without language restriction. The primary outcome was the time to the presence of bowel sounds and the time to the first passage of flatus. Cochrane's risk of bias tool was used to assess the risk of bias in included studies. Results: Nine studies with a total of 1011 patients were included. Overall, three studies were categorized as having a low risk of bias, three had some concerns, and three exhibited a high risk of bias. The time to the presence of bowel sounds (mean difference [MD] -2.66 h, 95% confidence interval [CI] -3.68 to -1.64, p < 0.00001) and time to the first passage of flatus (MD -4.20 h, 95% CI -5.79 to -2.61, p < 0.00001) was significantly shorter in the gum-chewing group. There was no statistical difference between the two groups with regard to the time to the first defecation (MD -6.52 h, 95% CI -15.70 to 2.66, p = 0.16), time to the first postoperative mobilization (MD 24.05 min, 95% CI -38.16 to 86.26, p = 0.45), postoperative ileus (MD 0.68, 95% CI 0.39 to 1.19, p = 0.17), and length of hospital stay (MD -0.05 day, 95% CI -0.14 to 0.04, p = 0.28). Conclusions: Gum chewing following laparoscopic gynecologic surgery appears to promote the recovery of gastrointestinal function, as evidenced by a reduced time to the presence of bowel sounds and the first passage of flatus.
Keywords: gum chewing; gynecology; laparoscopy.
Conflict of interest statement
The authors declare no competing interests.
Figures


References
Publication types
LinkOut - more resources
Full Text Sources
