

Is the Tendon-to-Groove Ratio Associated with Elevated Risk for LHB Tendon Disorders?-A New Approach of Preoperative MR-Graphic Analysis for Targeted Diagnosis of Tendinopathy of the Long Head of Biceps
- PMID: 38792401
- PMCID: PMC11121934
- DOI: 10.3390/jcm13102860
Is the Tendon-to-Groove Ratio Associated with Elevated Risk for LHB Tendon Disorders?-A New Approach of Preoperative MR-Graphic Analysis for Targeted Diagnosis of Tendinopathy of the Long Head of Biceps
Abstract
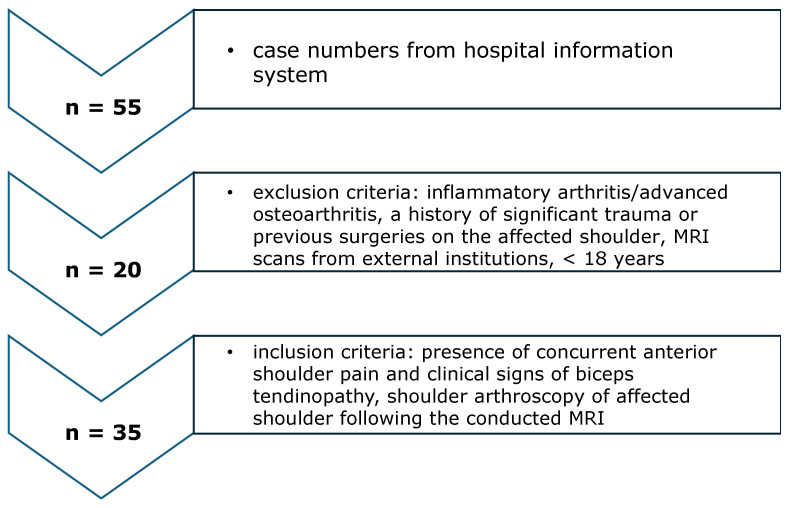
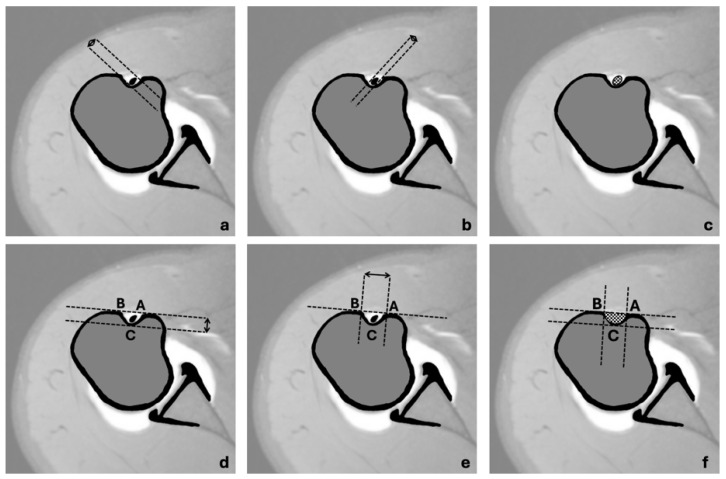
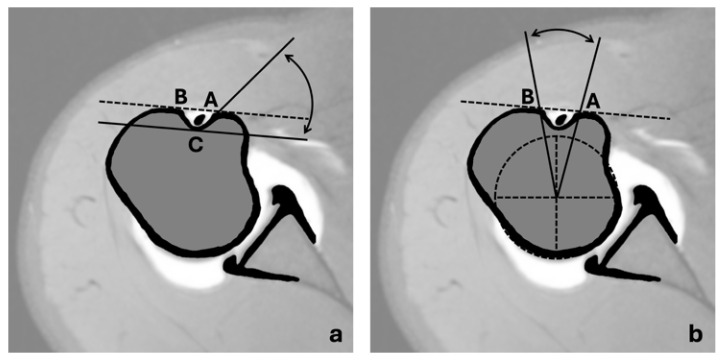
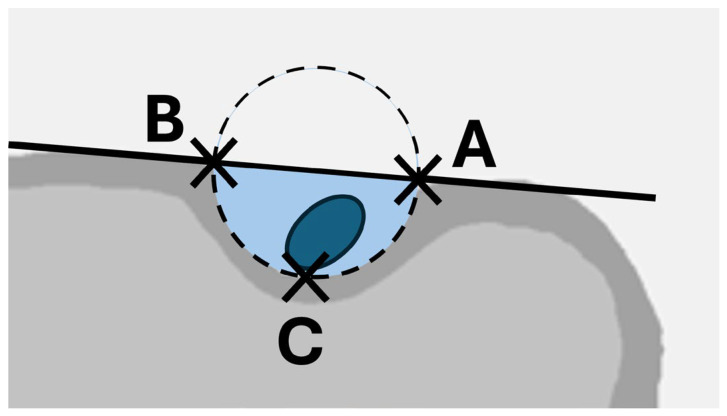
Background: Pathologies of the long head of the biceps (LHB) tendon are a common cause of anterior shoulder pain. While the influence of the anatomical morphology of the intertubercular groove (ITG) on the development of LHB tendon instability has been investigated with ambiguous results, the relationship of the LHB to ITG anatomy has not yet been considered in this context. The objective of this study was to reliably extract the tendon-to-groove ratio from MRI scans of symptomatic patients and examine its potential influence on the occurrence of certain causes for LHB-associated symptoms. Methods: In this retrospective study, preoperative MRI scans of 35 patients (mean age of 46 ± 14 years) presenting with anterior shoulder pain and clinical indications of LHB tendinopathy were analyzed in transversal planes. Long and short diameters of the LHB tendon and ITG were measured, cross-sectional areas of the LHB tendon and ITG were calculated from these measurements, and the ratio of cross-sectional areas (LHB/ITG) was introduced. All measurements were repeated independently by three investigators and inter-rater reliability was assessed using intraclass correlation coefficient (ICC). Thereafter, tendon-to-groove ratios were compared in patients with and without intraoperative signs of LHB tendon instability. Results: All patients exhibited intraoperative signs of LHB tendinitis, with additional findings including pulley lesions and SLAP lesions. Analysis revealed variations in the dimensions of the LHB tendon and ITG cross sections, with the tendon-to-groove ratio decreasing from 37% at the pulley to 31% at the deepest point of the sulcus. Very good inter-rater reliability was observed for all measurements. The tendon-to-groove ratio did not significantly differ (p > 0.05) in patients with or without pulley lesions or SLAP lesions. Conclusions: Our study introduced the novel parameter of the tendon-to-groove ratio of cross-sectional areas as a reproducible parameter for the description of local anatomy in the field of targeted diagnosis of LHB tendon disorders. While our findings do not yet support the predictive value of the tendon-to-groove ratio, they underscore the importance of further research with larger cohorts and control groups to validate these observations.
Keywords: arthroscopy; biceps tendon; intertubercular groove; pulley lesions; shoulder.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
[Tendinitis of the long head of biceps tendon associated with lesions of the "biceps reflection pulley"].Sportverletz Sportschaden. 2003 Jun;17(2):75-9. doi: 10.1055/s-2003-40132. Sportverletz Sportschaden. 2003. PMID: 12817319 German.
-
Biceps Pulley Lesions: Diagnostic Accuracy of Nonarthrographic Shoulder MRI and the Value of Various Diagnostic Signs.J Magn Reson Imaging. 2024 Apr;59(4):1299-1311. doi: 10.1002/jmri.29004. Epub 2023 Sep 7. J Magn Reson Imaging. 2024. PMID: 37675811
-
Shear wave elastography correlates to degeneration and stiffness of the long head of the biceps tendon in patients undergoing tenodesis with arthroscopic shoulder surgery.J Shoulder Elbow Surg. 2024 Jan;33(1):e31-e41. doi: 10.1016/j.jse.2023.05.014. Epub 2023 Jun 14. J Shoulder Elbow Surg. 2024. PMID: 37327988
-
Methods to analyse the long head of the biceps in the management of distal ruptures of the supraspinatus tendon. Part 1: the concept of the "biceps box": dynamic rotator interval approach. Incidence of lesions of the long head of the biceps tendon.Orthop Traumatol Surg Res. 2023 Dec;109(8S):103669. doi: 10.1016/j.otsr.2023.103669. Epub 2023 Jul 28. Orthop Traumatol Surg Res. 2023. PMID: 37517471 Review.
-
Injuries to the Biceps Pulley.Clin Sports Med. 2016 Jan;35(1):19-27. doi: 10.1016/j.csm.2015.08.003. Epub 2015 Sep 26. Clin Sports Med. 2016. PMID: 26614466 Review.
References
LinkOut - more resources
Full Text Sources
