

The Importance of In Vivo Reflectance Confocal Microscopy in a Case of Desmoplastic Melanoma
- PMID: 38792595
- PMCID: PMC11122514
- DOI: 10.3390/life14050574
The Importance of In Vivo Reflectance Confocal Microscopy in a Case of Desmoplastic Melanoma
Abstract
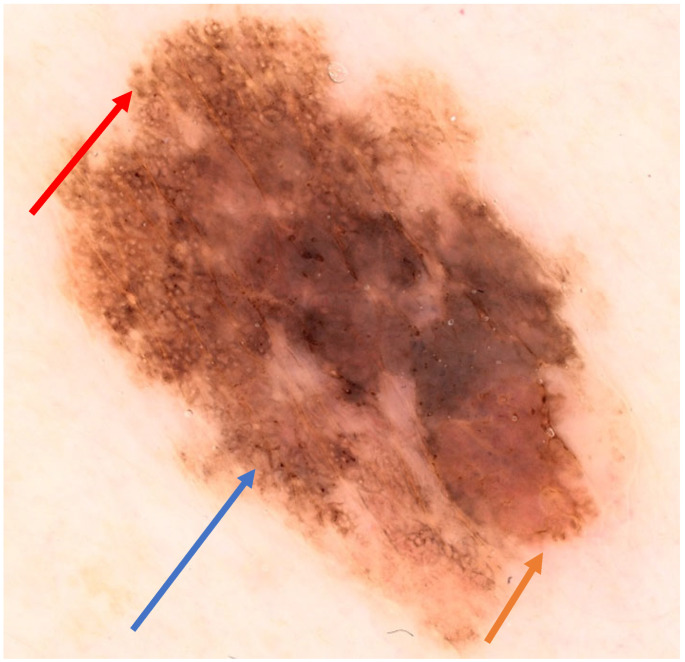
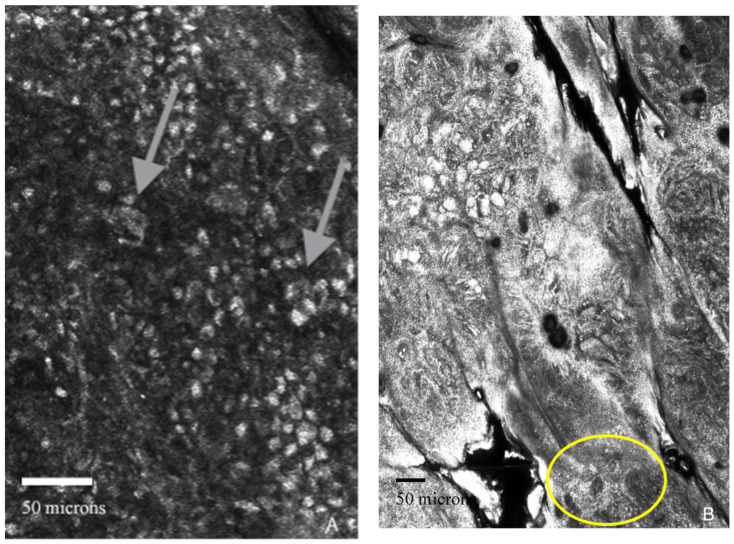
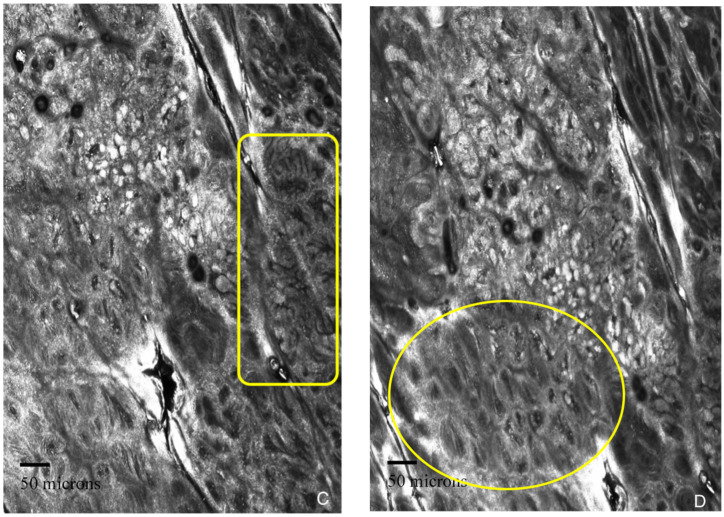
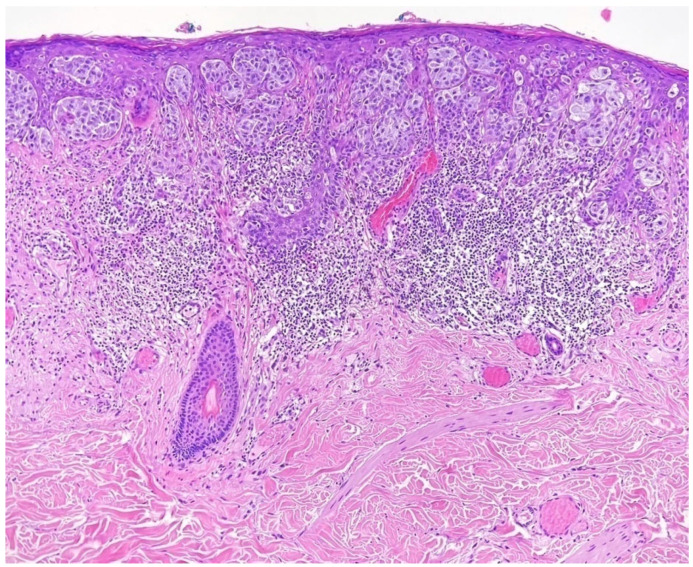
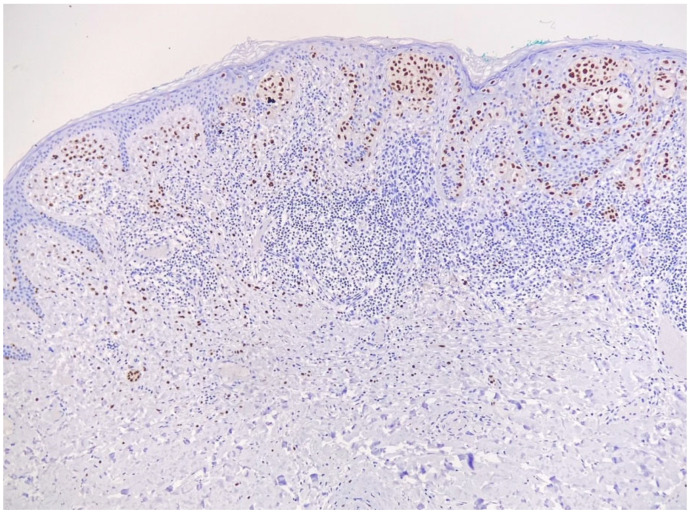
Desmoplastic melanoma accounts for 5% of all cases of melanoma, but its diagnosis can be difficult due to its frequent clinical presentation with amelanotic lesions. Histologically, spindled melanocytes surrounded by a collagenous stroma are observed. Compared with other types of melanoma, the desmoplastic types presents greater local aggression, and is more prone to local recurrence, but has a lower risk of lymph node metastasis. Early detection, accurate staging, and proper surgical management are the main factors associated with higher survival rates in melanoma patients. Reflectance confocal microscopy (RCM) has proven to be a valuable imaging tool in the diagnosis of skin neoplasms, being useful for orientating practitioners towards the diagnosis of melanoma and indicating the necessity of performing a diagnostic biopsy. We present the case of 52-year-old woman, who presented to the dermatology department with an irregular, dark-colored plaque in the right deltoid region. Dermoscopy showed asymmetry with an atypical network and some areas of regression. RCM revealed pagetoid cells in the upper epidermis, cell atypia, non-edged papillae, dermal inflammation, and nucleated cells in the dermis, which are highly suggestive of melanoma. A biopsy was also performed. A histopathology exam confirmed the diagnosis of superficially spreading melanoma with a desmoplastic component, and revealed a Breslow index of 0.9 mm, Clark level IV, an absence of mitoses, angiolymphatic invasion and regression, and complete excision. The CT and PET-CT scans were negative. A biopsy of the axillary sentinel lymph node was conducted, with a negative result obtained, establishing the IB stage of the disease. The patient will remain under follow-up to look for a recurrence or a new primary melanoma.
Keywords: dermoscopy; desmoplastic melanoma; diagnosis; histopathological subtype; prognostic; reflectance confocal microscopy.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

Similar articles
-
Role of In Vivo Reflectance Confocal Microscopy in the Analysis of Melanocytic Lesions.Acta Dermatovenerol Croat. 2018 Apr;26(1):64-67. Acta Dermatovenerol Croat. 2018. PMID: 29782304 Review.
-
Desmoplastic Melanoma as a Diagnostic Pitfall.Acta Dermatovenerol Croat. 2020 Jul;28(1):49-50. Acta Dermatovenerol Croat. 2020. PMID: 32650855
-
Reflectance confocal microscopy in the diagnosis of partially and completely amelanotic melanoma: report on seven cases.J Eur Acad Dermatol Venereol. 2013 Jan;27(1):e42-52. doi: 10.1111/j.1468-3083.2012.04465.x. Epub 2012 Feb 10. J Eur Acad Dermatol Venereol. 2013. PMID: 22324783
-
Morphological classification of melanoma metastasis with reflectance confocal microscopy.J Eur Acad Dermatol Venereol. 2019 Apr;33(4):676-685. doi: 10.1111/jdv.15329. Epub 2018 Dec 4. J Eur Acad Dermatol Venereol. 2019. PMID: 30394598
-
Amelanotic melanoma: Clinical presentation, diagnosis, and management.Clin Dermatol. 2025 Jan-Feb;43(1):10-15. doi: 10.1016/j.clindermatol.2025.01.009. Epub 2025 Feb 1. Clin Dermatol. 2025. PMID: 39900311 Review.
References
-
- Garbe C., Amaral T., Peris K., Hauschild A., Arenberger P., Basset-Seguin N., Bastholt L., Bataille V., del Marmol V., Dréno B., et al. European Consensus-Based Interdisciplinary Guideline for Melanoma. Part 1: Diagnostics: Update 2022. Eur. J. Cancer. 2022;170:236–255. doi: 10.1016/j.ejca.2022.03.008. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
