

Coronary Computed Tomography Angiography-Derived Modified Duke Index Is Associated with Peri-Coronary Fat Attenuation Index and Predicts Severity of Coronary Inflammation
- PMID: 38792949
- PMCID: PMC11123489
- DOI: 10.3390/medicina60050765
Coronary Computed Tomography Angiography-Derived Modified Duke Index Is Associated with Peri-Coronary Fat Attenuation Index and Predicts Severity of Coronary Inflammation
Abstract
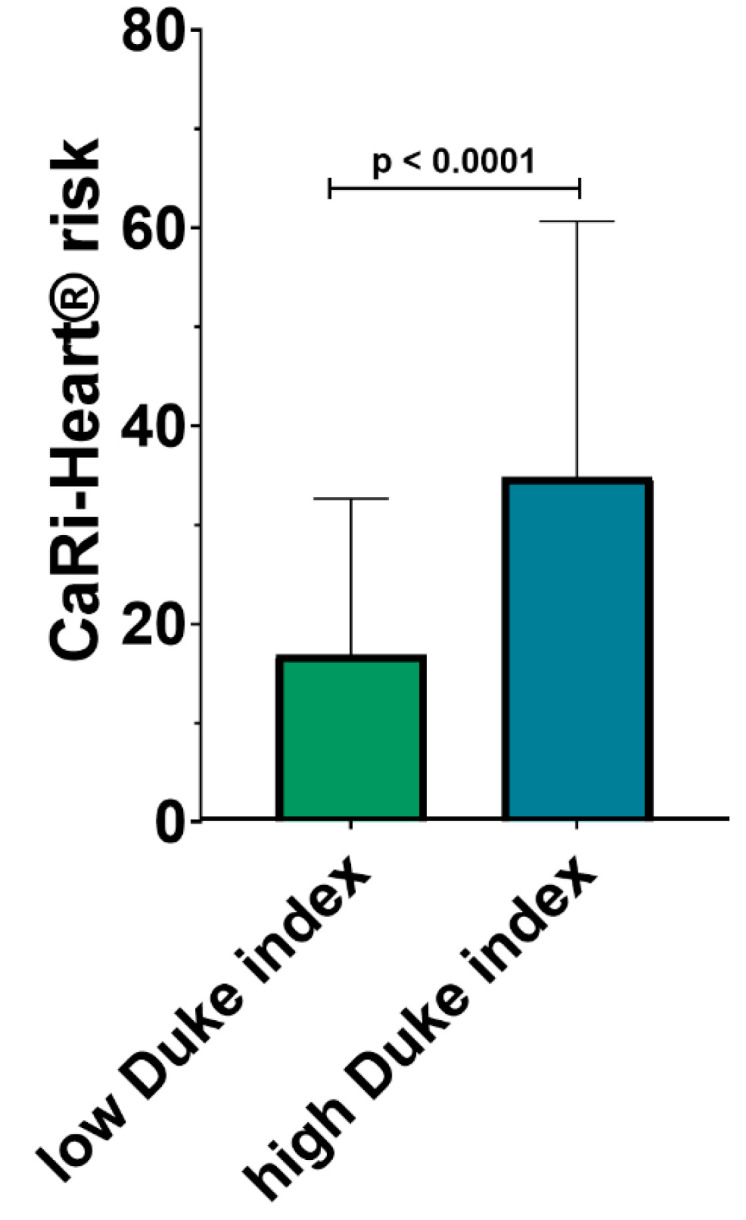
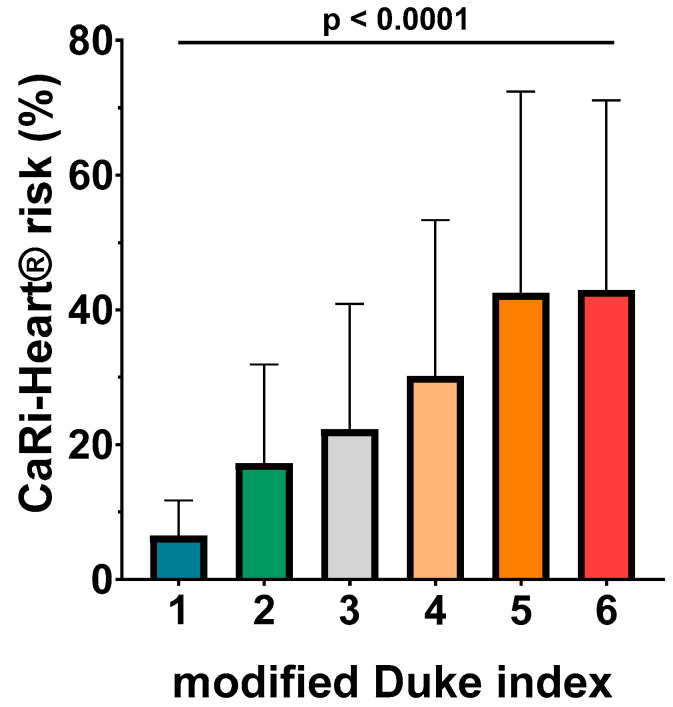
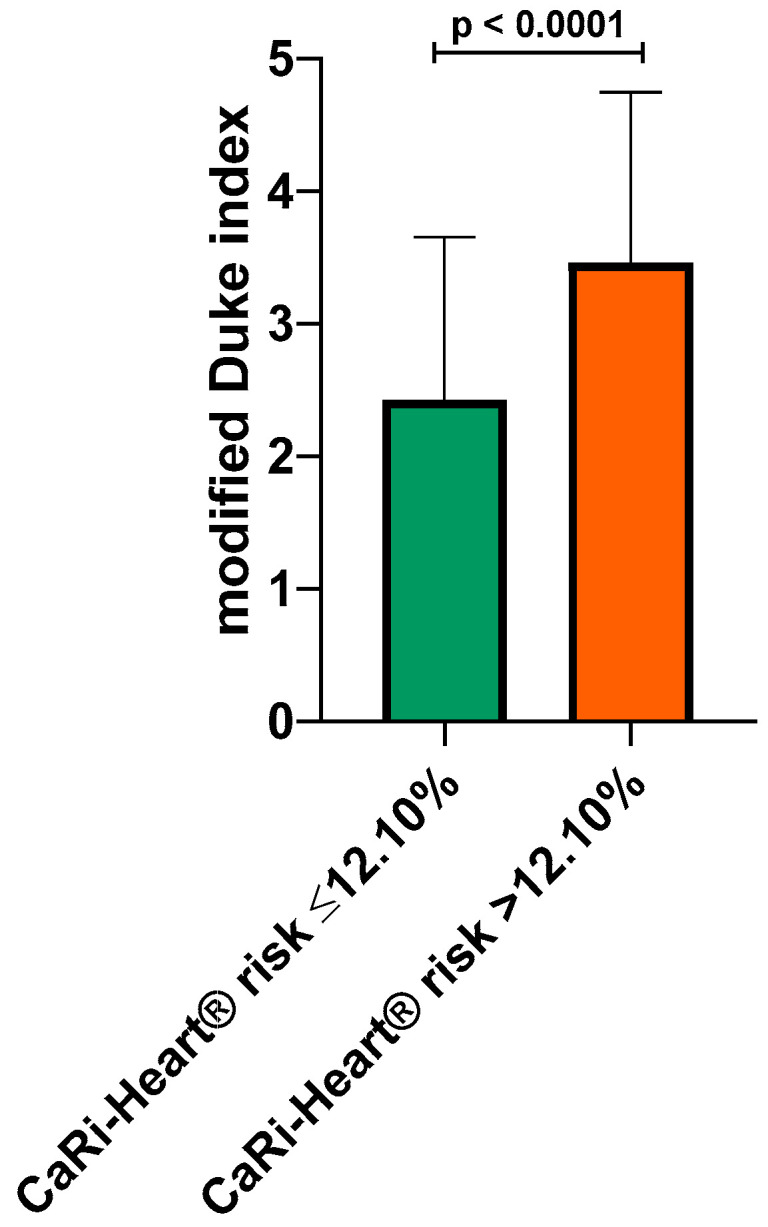
Background and Objectives: The modified Duke index derived from coronary computed tomography angiography (CCTA) was designed to predict cardiovascular outcomes based on the severity of coronary stenosis. However, it does not take into consideration the presence or severity of peri-coronary inflammation. The peri-coronary fat attenuation index (FAI) is a novel imaging marker determined by CCTA which reflects the degree of inflammation in the coronary tree in patients with coronary artery disease. To assess the association between the modified Duke index assessed by CCTA, cardiovascular risk factors, and peri-coronary inflammation in the coronary arteries of patients with coronary artery disease. Materials and Methods: One hundred seventy-two patients who underwent CCTA for typical angina were assigned into two groups based on the modified Duke index: group 1-patients with low index, ≤3 (n = 107), and group 2-patients with high index, >3 (n = 65). Demographic, clinical, and CCTA data were collected for all patients, and FAI analysis of coronary inflammation was performed. Results: Patients with increased values of the modified Duke index were significantly older compared to those with a low index (61.83 ± 9.89 vs. 64.78 ± 8.9; p = 0.002). No differences were found between the two groups in terms of gender distribution, hypertension, hypercholesterolemia, or smoking history (all p > 0.5). The FAI score was significantly higher in patients from group 2, who presented a significantly higher score of inflammation compared to the patients in group 1, especially at the level of the right coronary artery (FAI score, 20.85 ± 15.80 vs. 14.61 ± 16.66; p = 0.01 for the right coronary artery, 13.85 ± 8.04 vs. 10.91 ± 6.5; p = 0.01 for the circumflex artery, 13.26 ± 10.18 vs. 11.37 ± 8.84; p = 0.2 for the left anterior descending artery). CaRi-Heart® analysis identified a significantly higher risk of future events among patients with a high modified Duke index (34.84% ± 25.86% vs. 16.87% ± 15.80%; p < 0.0001). ROC analysis identified a cut-off value of 12.1% of the CaRi-Heart® risk score for predicting a high severity of coronary lesions, with an AUC of 0.69. Conclusions: The CT-derived modified Duke index correlates well with local perilesional inflammation as assessed using the FAI score at different levels of the coronary circulation.
Keywords: CariHeart; cardiac computed tomography; coronary stenosis; fat attenuation index; inflammation.
Conflict of interest statement
The authors declare no conflict of interest.
Figures


References
-
- Bordi L., Opincariu D., Benedek T., Kovács I., Parajkó Z., Márton E., Gerculy R., Benedek I. Left Atrial Volume Quantified by MSCT Predicts Emergency Hospitalizations for AF and Arrhythmia Recurrence after Catheter Ablation. J. Cardiovasc. Emergencies. 2023;9:24–31. doi: 10.2478/jce-2023-0004. - DOI
-
- Min J.K., Shaw L.J., Devereux R.B., Okin P.M., Weinsaft J.W., Russo D.J., Lippolis N.J., Berman D.S., Callister T.Q. Prognostic value of multidetector coronary computed tomographic angiography for prediction of all-cause mortality. J. Am. Coll. Cardiol. 2007;50:1161–1170. doi: 10.1016/j.jacc.2007.03.067. - DOI - PubMed
-
- Rodean I.P., Lazăr L., Halațiu V.B., Biriș C., Benedek I., Benedek T. Periodontal Disease Is Associated with Increased Vulnerability of Coronary Atheromatous Plaques in Patients Undergoing Coronary Computed Tomography Angiography-Results from the Atherodent Study. J. Clin. Med. 2021;10:1290. doi: 10.3390/jcm10061290. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
