

Quality-of-Life Assessment in Children with Mild to Moderate Bronchial Asthma
- PMID: 38792954
- PMCID: PMC11122762
- DOI: 10.3390/medicina60050771
Quality-of-Life Assessment in Children with Mild to Moderate Bronchial Asthma
Abstract
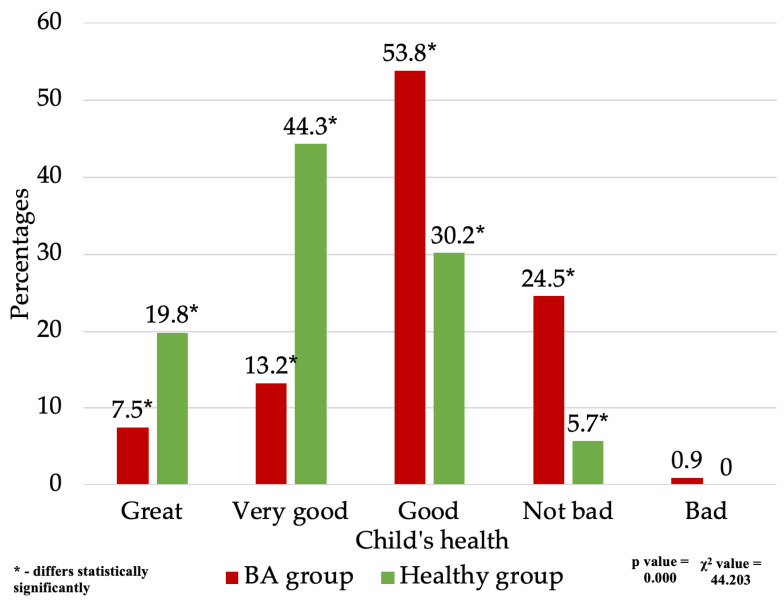
Background and Objectives: Assess the quality of life of children aged 2-10 with mild to moderate bronchial asthma. To evaluate the general health condition of children with mild and moderate severity bronchial asthma. To determine health changes in children with mild- and moderate-severity bronchial asthma as they grow older. To evaluate the impact of mild- and moderate-severity bronchial asthma on children's daily and social activities, physical health, emotional state, and general well-being. Materials and Methods: A comparative cross-sectional study was conducted in March-June 2020. Parents or guardians of 2-10-year-old children without bronchial asthma and children with mild to moderate bronchial asthma were interviewed after receiving their written informed consent. The questionnaire was based on the standardized quality-of-life quiz SF-36. A total of 248 questionnaires were collected-106 from the parents or guardians of children with bronchial asthma and 142 from parents/guardians of children without bronchial asthma. For further analysis, 106 children without bronchial asthma and with no chronic conditions were selected. Quantitative variables were compared using the Mann-Whitney U test and qualitative data using the chi-square (χ2) criteria. Quantitative data were described by giving means, medians, and standard deviations (SD); qualitative features by giving relative frequencies. Statistical data were analyzed using SPSS and Excel 2020. Results: Children with mild and moderate asthma exhibit poorer health compared to their healthy counterparts. Only 20.7% of respondents with asthma reported excellent or very good health, contrasting with 64.1% of healthy children (p < 0.001). As children with asthma age, their general condition improves, with 46.2% showing improvement in the past year, while 42.5% of healthy children had a stable condition (p < 0.05). In various activities, children with asthma face more constraints than healthy children (p < 0.05), including energetic activities (sick-59.5%; healthy-10.3%), moderate activities (sick-24.5%; healthy-4.7%), climbing stairs (sick-22.7%; healthy-3.8%), and walking over 100 m (sick-9.4%; healthy-0%). Children with asthma are more likely to experience exhaustion, anxiety, tiredness, lack of energy, and restraint in public activities (p < 0.05). Conclusions: Parents/caregivers of children with mild to moderate bronchial asthma rate their health worse than those of healthy children do. As children with mild to moderate bronchial asthma grow, the disease impact on their overall well-being decreases. Children with mild to moderate bronchial asthma, compared to healthy children, experience more limitations in vigorous or moderate activities; face more difficulties climbing stairs or walking more than 100 m; frequently feel exhaustion, anxiety, fatigue, or lack of energy; and encounter restrictions in social activities.
Keywords: bronchial asthma; child; children; pediatric patient; quality of life.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures


References
-
- GBD 2016 Disease and Injury Incidence and Prevalence Collaborators Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390:1211–1259. doi: 10.1016/S0140-6736(17)32154-2. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
