

Do Precision and Personalised Nutrition Interventions Improve Risk Factors in Adults with Prediabetes or Metabolic Syndrome? A Systematic Review of Randomised Controlled Trials
- PMID: 38794717
- PMCID: PMC11124316
- DOI: 10.3390/nu16101479
Do Precision and Personalised Nutrition Interventions Improve Risk Factors in Adults with Prediabetes or Metabolic Syndrome? A Systematic Review of Randomised Controlled Trials
Abstract
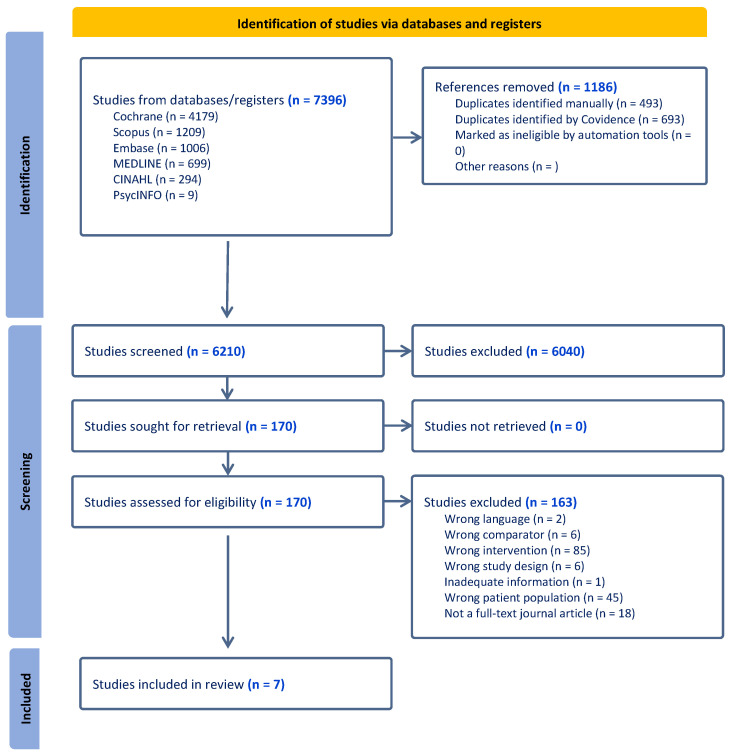
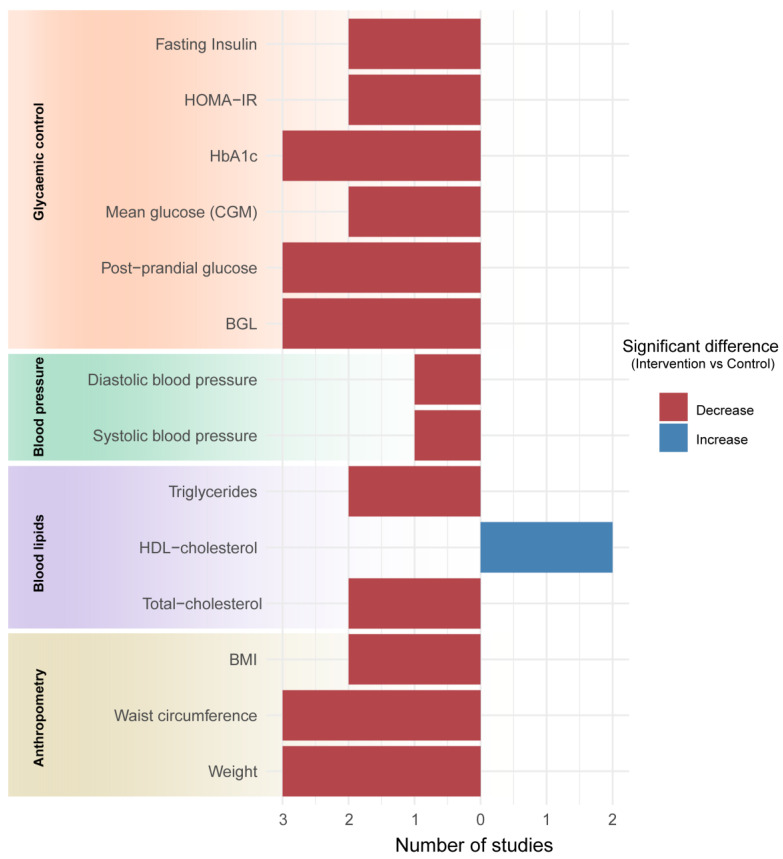
This review aimed to synthesise existing literature on the efficacy of personalised or precision nutrition (PPN) interventions, including medical nutrition therapy (MNT), in improving outcomes related to glycaemic control (HbA1c, post-prandial glucose [PPG], and fasting blood glucose), anthropometry (weight, BMI, and waist circumference [WC]), blood lipids, blood pressure (BP), and dietary intake among adults with prediabetes or metabolic syndrome (MetS). Six databases were systematically searched (Scopus, Medline, Embase, CINAHL, PsycINFO, and Cochrane) for randomised controlled trials (RCTs) published from January 2000 to 16 April 2023. The Academy of Nutrition and Dietetics Quality Criteria were used to assess the risk of bias. Seven RCTs (n = 873), comprising five PPN and two MNT interventions, lasting 3-24 months were included. Consistent and significant improvements favouring PPN and MNT interventions were reported across studies that examined outcomes like HbA1c, PPG, and waist circumference. Results for other measures, including fasting blood glucose, HOMA-IR, blood lipids, BP, and diet, were inconsistent. Longer, more frequent interventions yielded greater improvements, especially for HbA1c and WC. However, more research in studies with larger sample sizes and standardised PPN definitions is needed. Future studies should also investigate combining MNT with contemporary PPN factors, including genetic, epigenetic, metabolomic, and metagenomic data.
Keywords: medical nutrition therapy; metabolic syndrome; personalized nutrition; precision nutrition; prediabetes; randomized controlled trial; systematic review.
Conflict of interest statement
C.E.C. is funded by an Australian National Health and Medical Research Council Leadership Investigator Grant (APP2009340). The authors declare that they have no conflicts of interest to disclose.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
