

REAL-Colon: A dataset for developing real-world AI applications in colonoscopy
- PMID: 38796533
- PMCID: PMC11127922
- DOI: 10.1038/s41597-024-03359-0
REAL-Colon: A dataset for developing real-world AI applications in colonoscopy
Abstract
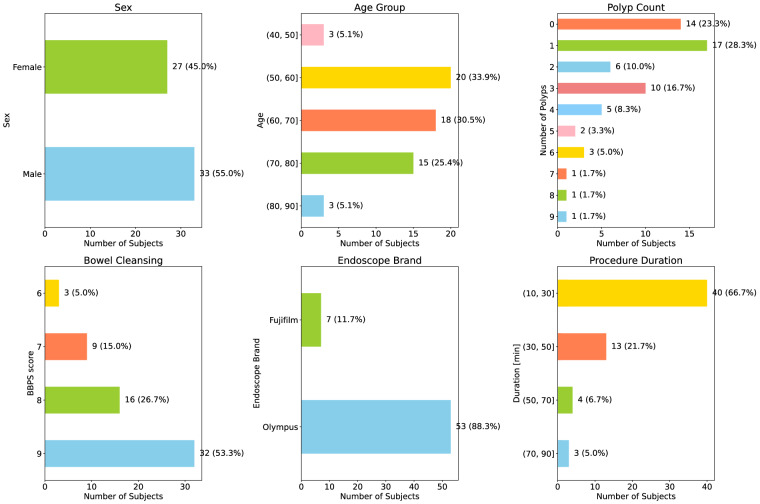
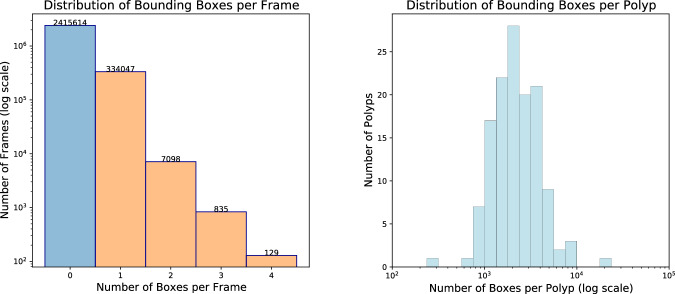
Detection and diagnosis of colon polyps are key to preventing colorectal cancer. Recent evidence suggests that AI-based computer-aided detection (CADe) and computer-aided diagnosis (CADx) systems can enhance endoscopists' performance and boost colonoscopy effectiveness. However, most available public datasets primarily consist of still images or video clips, often at a down-sampled resolution, and do not accurately represent real-world colonoscopy procedures. We introduce the REAL-Colon (Real-world multi-center Endoscopy Annotated video Library) dataset: a compilation of 2.7 M native video frames from sixty full-resolution, real-world colonoscopy recordings across multiple centers. The dataset contains 350k bounding-box annotations, each created under the supervision of expert gastroenterologists. Comprehensive patient clinical data, colonoscopy acquisition information, and polyp histopathological information are also included in each video. With its unprecedented size, quality, and heterogeneity, the REAL-Colon dataset is a unique resource for researchers and developers aiming to advance AI research in colonoscopy. Its openness and transparency facilitate rigorous and reproducible research, fostering the development and benchmarking of more accurate and reliable colonoscopy-related algorithms and models.
© 2024. The Author(s).
Conflict of interest statement
C.B., P.S., and A.C. are affiliated with Cosmo Intelligent Medical Devices, the developer of the GI Genius medical device. C.H. is consultant for Medtronic and Fujifilm.
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
