

Long-term kidney outcomes of semaglutide in obesity and cardiovascular disease in the SELECT trial
- PMID: 38796653
- PMCID: PMC11271413
- DOI: 10.1038/s41591-024-03015-5
Long-term kidney outcomes of semaglutide in obesity and cardiovascular disease in the SELECT trial
Abstract
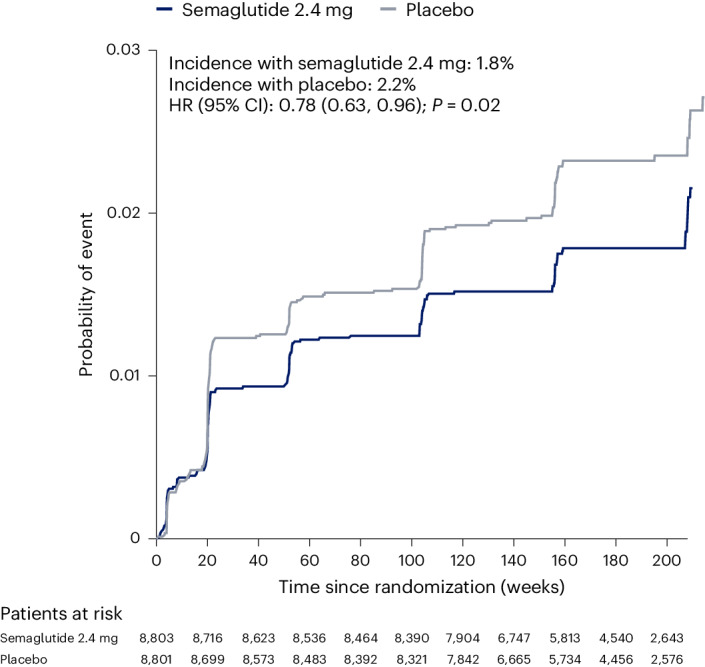
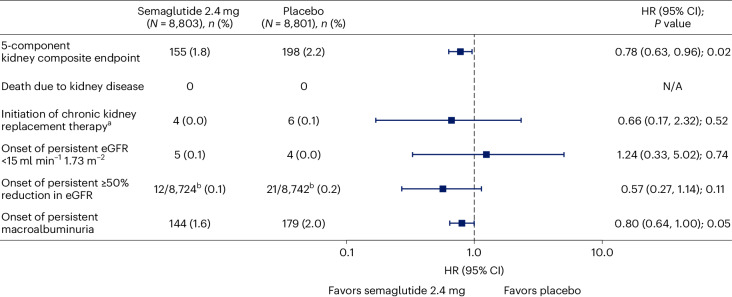
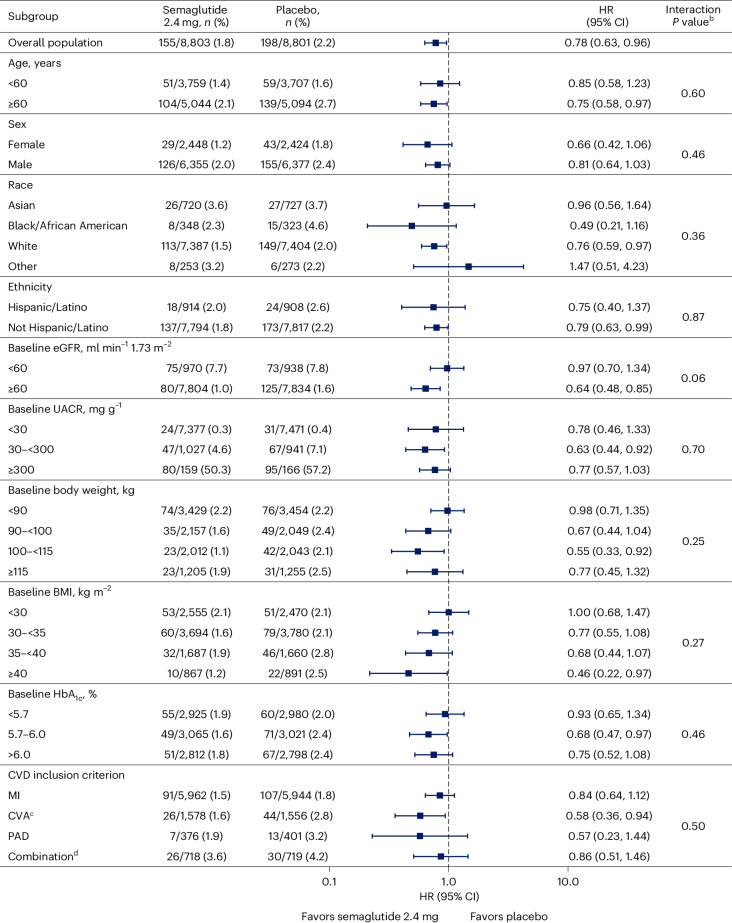
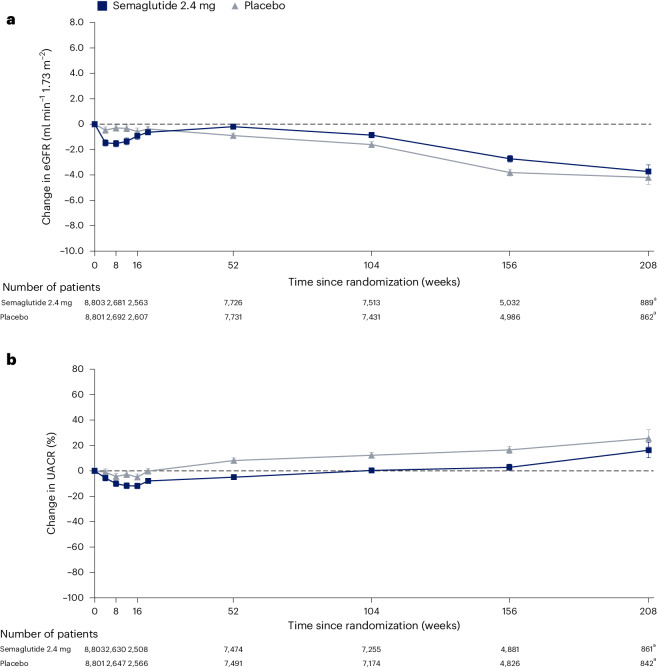
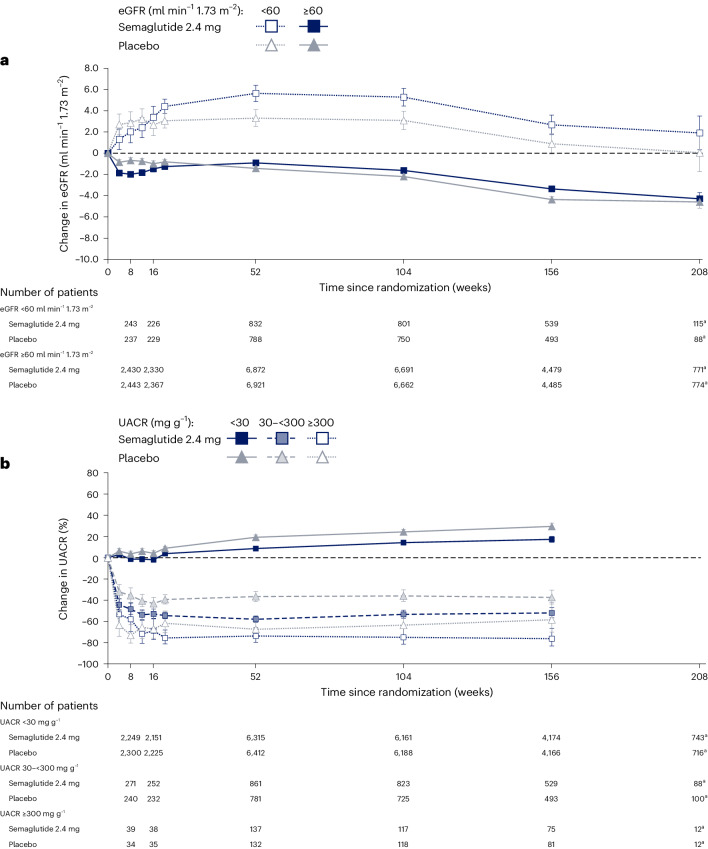
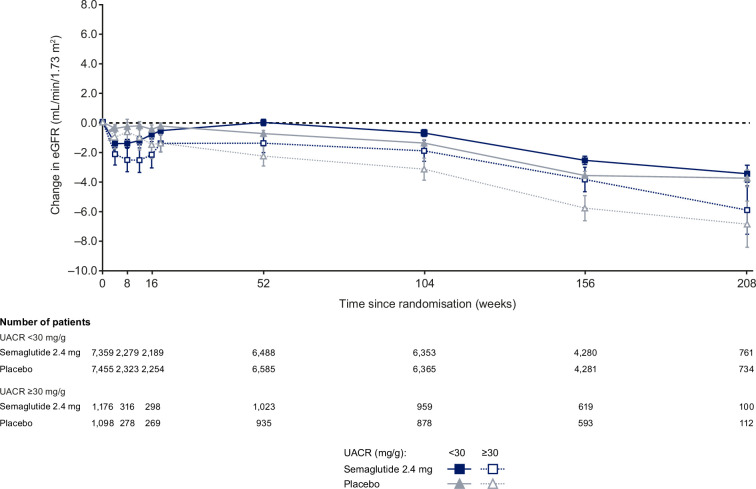
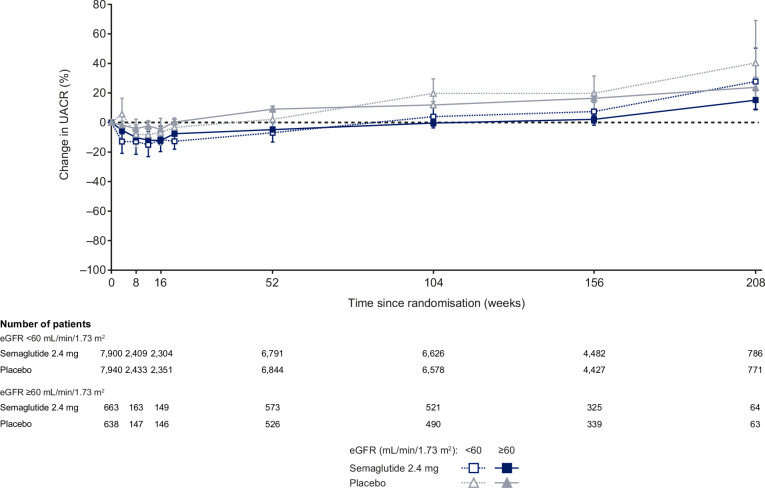
The SELECT trial previously reported a 20% reduction in major adverse cardiovascular events with semaglutide (n = 8,803) versus placebo (n = 8,801) in patients with overweight/obesity and established cardiovascular disease, without diabetes. In the present study, we examined the effect of once-weekly semaglutide 2.4 mg on kidney outcomes in the SELECT trial. The incidence of the pre-specified main composite kidney endpoint (death from kidney disease, initiation of chronic kidney replacement therapy, onset of persistent estimated glomerular filtration rate (eGFR) < 15 ml min-1 1.73 m-2, persistent ≥50% reduction in eGFR or onset of persistent macroalbuminuria) was lower with semaglutide (1.8%) versus placebo (2.2%): hazard ratio (HR) = 0.78; 95% confidence interval (CI) 0.63, 0.96; P = 0.02. The treatment benefit at 104 weeks for eGFR was 0.75 ml min-1 1.73 m-2 (95% CI 0.43, 1.06; P < 0.001) overall and 2.19 ml min-1 1.73 m-2 (95% CI 1.00, 3.38; P < 0.001) in patients with baseline eGFR <60 ml min-1 1.73 m-2. These results suggest a benefit of semaglutide on kidney outcomes in individuals with overweight/obesity, without diabetes.ClinicalTrials.gov identifier: NCT03574597 .
© 2024. The Author(s).
Conflict of interest statement
P.M.B. declares being an employee of and stakeholder in Novo Nordisk. H.M.C. declares serving on advisory panels for Novo Nordisk and Bayer; receiving research funding from Sanofi, Roche and IQVIA; receiving grants from the Chief Scientist Office, Diabetes UK, the European Commission, the Juvenile Diabetes Research Foundation and the Medical Research Council (MRC); serving on a speaker’s bureau for Novo Nordisk; and holding stock in Roche and Bayer. J.D. declares having received consulting honoraria from Amgen, Boehringer Ingelheim, Merck, Pfizer, Aegerion, Novartis, Sanofi, Takeda, Novo Nordisk and Bayer and research grants from the British Heart Foundation, the MRC, the National Institute for Health and Care Research, Public Health England, Merck Sharp & Dohme (MSD), Pfizer, Aegerion, Colgate and Roche. K.B.-F. declares being an employee of and stockholder in Novo Nordisk. S.E.K., for the period over which SELECT was conducted, declares receiving advisory board/consulting fees from AltPep, Bayer, Boehringer Ingelheim, Casma Therapeutics, Eli Lilly, Intarcia, Merck, Novo Nordisk, Oramed, Pfizer and Third Rock Ventures. T.I. declares being an employee of and stockholder in Novo Nordisk. I.L. declares having received research grants from Boehringer Ingelheim, Merck, Mylan Pharmaceuticals, Novo Nordisk, Pfizer and Sanofi US Services; service as a consultant for AstraZeneca, Bayer Healthcare Pharmaceuticals, Biomea Fusion, Boehringer Ingelheim, Carmot, Eli Lilly, Intarcia, Intercept Pharmaceuticals, Janssen Global Services, Johnson & Johnson Medical Devices & Diagnostics Group–Latin America, MannKind Corporation, Merck, Novo Nordisk, Pfizer, Sanofi US Services, Shionogi, Structure Therapeutics, Target Pharma, Valeritas and Zealand Pharma A/S; and having received travel expenses from Boehringer Ingelheim, Eli Lilly, Johnson & Johnson Medical Devices & Diagnostics Group– Latin America, Novo Nordisk, Sanofi US Services and Zealand Pharma A/S. A.M.L. declares having received honoraria from Akebia, Alnylam, Ardelyx, Becton Dickinson, Brainstorm Cell, Eli Lilly, Endologix, FibroGen, GlaxoSmithKline, Intarcia, Medtronic, Neovasc, Novo Nordisk, Provention Bio and ReCor and consulting activities and research funding to his institution from AbbVie, AstraZeneca, CSL Behring, Eli Lilly, Esperion and Novartis. J.F.E.M. reports personal fees from AstraZeneca, Amgen, Braun, ACI and Fresenius; grants and personal fees from Celgene; personal fees from Gambro; grants from the European Union and McMaster University (Canada); grants and personal fees from AbbVie; personal fees from Medice; grants and personal fees from Novo Nordisk, Roche and Sandoz; and personal fees from Lanthio, Sanifit, Relypsa and ZS Pharma, all outside the submitted work. K.N. declares having received honoraria from AstraZeneca, Bayer Yakuhin, Boehringer Ingelheim Japan, Daiichi Sankyo, Eli Lilly Japan, Kowa, Mitsubishi Tanabe Pharma, Mochida Pharmaceutical, MSD, Novartis Pharma, Novo Nordisk Pharma, Ono Pharmaceutical, Otsuka and Tsumura; research grants from Astellas, Bayer Yakuhin, Boehringer Ingelheim Japan, Fuji Yakuhin, Mitsubishi Tanabe Pharma, Mochida Pharmaceutical and Novartis Pharma; and scholarships from Abbott, Boehringer Ingelheim Japan, Daiichi Sankyo, Mitsubishi Tanabe Pharma and Teijin Pharma. A.P. declares having received research grants and personal fees during the study from Novo Nordisk. J.P. declares having received consulting honoraria from Altimmune, Amgen, Esperion Therapeutics, Merck, MJH Life Sciences, Novartis and Novo Nordisk and having received a grant, paid to his institution, from Boehringer Ingelheim. J.P. also holds the position of Director, Preventive Cardiology, at Brigham and Women’s Hospital. L.R. declares research grants from Amgen, Bristol Myers Squibb, the Erling Persson Foundation, Novo Nordisk and the Swedish Heart Lung Foundation and lecture/consultant honoraria from Bayer, Eli Lilly and Novo Nordisk. N.R. declares being an employee of and stockholder in Novo Nordisk. K.R.T. declares receiving research grants from the National Institutes of Health and Travere Therapeutics and consultancy and/or speaker fees from Bayer, Boehringer Ingelheim, Eli Lilly and Novo Nordisk. J.P.H.W. is contracted via the University of Liverpool (no personal payment) to undertake consultancy for Altimmune, AstraZeneca, Boehringer Ingelheim, Cytoki, Eli Lilly, Napp, Novo Nordisk, Menarini, Pfizer, Rhythm Pharmaceuticals, Sanofi, Saniona, Tern, Shionogi and Ysopia and declares personal honoraria/lecture fees from AstraZeneca, Boehringer Ingelheim, Medscape, Menarini, Napp, Novo Nordisk and Rhythm.
Figures
Comment in
-
A pre-specified analysis of the SELECT trial suggests a kidney benefit of semaglutide in patients without diabetes.Nat Rev Nephrol. 2024 Aug;20(8):493. doi: 10.1038/s41581-024-00865-7. Nat Rev Nephrol. 2024. PMID: 38956439 No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
