

IL-6 inhibition with clazakizumab in patients receiving maintenance dialysis: a randomized phase 2b trial
- PMID: 38796655
- PMCID: PMC11333272
- DOI: 10.1038/s41591-024-03043-1
IL-6 inhibition with clazakizumab in patients receiving maintenance dialysis: a randomized phase 2b trial
Erratum in
-
Author Correction: IL-6 inhibition with clazakizumab in patients receiving maintenance dialysis: a randomized phase 2b trial.Nat Med. 2024 Aug;30(8):2373. doi: 10.1038/s41591-024-03156-7. Nat Med. 2024. PMID: 38961226 Free PMC article. No abstract available.
Abstract
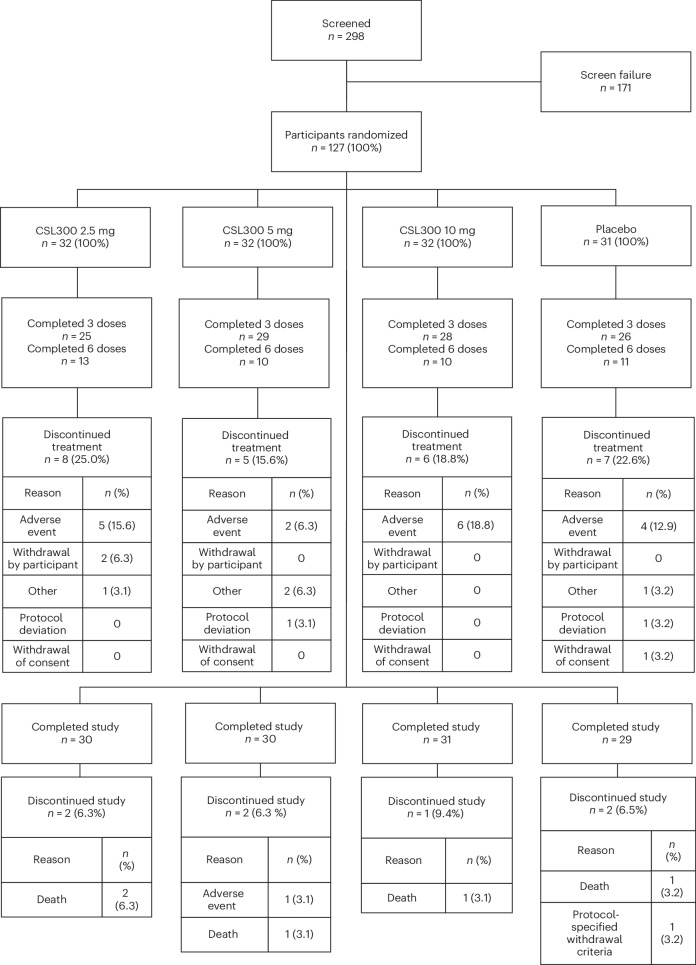
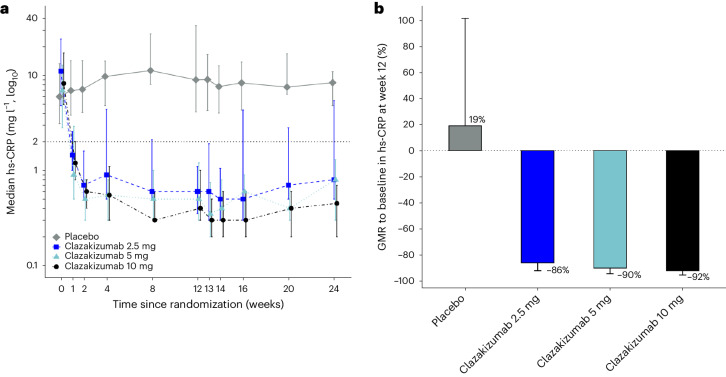
Inflammation mediated by interleukin-6 (IL-6) is strongly associated with cardiovascular risk. Here we evaluated clazakizumab, a monoclonal antibody targeting the IL-6 ligand, in a phase 2b dose-finding study. Adults with cardiovascular disease and/or diabetes receiving maintenance dialysis with high-sensitivity C-reactive protein (hs-CRP) ≥ 2 mg l-1 at baseline were randomized to receive clazakizumab (2.5 mg, 5 mg or 10 mg, n = 32 per dose group) or placebo (n = 31) every 4 weeks. The primary endpoint was the change from baseline in hs-CRP to week 12, expressed as the geometric mean ratio. Clazakizumab treatment signficantly reduced serum hs-CRP concentrations at week 12 by 86%, 90% and 92% relative to placebo in patients randomized to 2.5 mg, 5 mg or 10 mg clazakizumab, respectively (all P < 0.0001), meeting the primary outcome. With regard to secondary endpoints, clazakizumab treatment reduced serum fibrinogen, amyloid A, secretory phospholipase A2, and lipoprotein(a) concentrations, as well as increased mean serum albumin concentrations at 12 weeks, relative to placebo. The proportion of patients who achieved hs-CRP < 2.0 mg l-1 was 79%, 82% and 79% in the 2.5 mg, 5 mg and 10 mg clazakizumab groups, respectively, compared with 0% of placebo-treated patients. With regard to safety, no cases of sustained grade 3 or 4 thrombocytopenia or neutropenia were observed. Serious infections were seen with similar frequency in the placebo, clazakizumab 2.5 mg and clazakizumab 5 mg groups, but were numerically more frequent in the clazakizumab 10 mg group. The results of this trial indicate that in patients receiving maintenance dialysis, clazakizumab reduced inflammatory biomarkers associated with cardiovascular events. ClinicalTrials.gov registration: NCT05485961 .
© 2024. The Author(s).
Conflict of interest statement
G.M.C. has served on the Board of Directors of Satellite Healthcare, a nonprofit dialysis provider. His institution (Stanford University) has received a grant from the trial sponsor, CSL Behring. G.M.C. has served as Chair or Cochair of Trial Steering Committees with Akebia, AstraZeneca, CSL Behring, Sanifit and Vertex. He has served as an Advisor to Alexion, Applaud, Ardelyx, CalciMedica, Calico, CloudCath, Durect, Eliaz Therapeutics, Miromatrix, Outset, Renibus and Unicycive. He has served as Chair or Member of Data Safety Monitoring Boards for clinical trials sponsored by Bayer, Mineralys and ReCor. A.M.C., M.H., R.C., J.M. and P.T. are employees of and hold stock in CSL Behring. E.V. is an employee of CSL Limited. G.M.F. received research grants from NIH, Bayer, BMS, Novartis, Daxor, Merck, Cytokinetics and CSL Behring. He has acted as a consultant to Novartis, BMS, Cytokinetics, Innolife, Boehringer Ingelheim, Abbott, Sanofi, Regeneron, Myovant, Sequana, Windtree Therapeutics and Whiteswell, and has served on clinical endpoint committees/data safety monitoring boards for Merck, Medtronic, EBR Systems, Rocket Pharma, V-Wave and LivaNova. B.F. has served in from CSL Behring. D.M.C. reports consultancy with Eli Lilly/Boehringer Ingelheim, AstraZeneca, Allena Pharmaceuticals (DSMB), Gilead, Novo Nordisk, GSK, Medtronic, Merck, CSL Behring, Zogenix, Renalytix and LG Chemical. He has received research funding from Medtronic, Gilead; Novo Nordisk; Amgen, Boehringer Ingelheim/Eli Lilly; and has held patents or royalties with UpToDate.com for authorship/editorials on reviews. C.M.G. receives research and consulting support from CSL Behring. S.G.G. received research grant support (for example, steering committee or data and safety monitoring committee) and/or speaker/consulting honoraria (for example, advisory boards) from CSL Behring, Alnylam, Amgen, Anthos Therapeutics, AstraZeneca, Bayer, Boehringer Ingelheim, Bristol Myers Squibb, CYTE Ltd., Daiichi Sankyo/American Regent, Eli Lilly, Esperion, Ferring Pharmaceuticals, HLS Therapeutics, Idorsia, JAMP Pharma, Merck, Novartis, Novo Nordisk A/C, Pendopharm/Pharmascience, Pfizer, Regeneron, Roche, Sanofi, Servier, Tolmar Pharmaceuticals and Valeo Pharma and salary support/honoraria from the Canadian Heart Failure Society, Canadian Heart Research Center and MD Primer, Canadian VIGOUR Center, Cleveland Clinic Coordinating Center for Clinical Research, Duke Clinical Research Institute, Jewish General Hospital\CIUSSS Center-Ouest-de-l’Ile-de-Montreal, New York University Clinical Coordinating Center, PERFUSE Research Institute, Peter Munk Cardiac Center Clinical Trials and Translation Unit, Ted Rogers Heart Center and TIMI Study Group (Brigham Health). M.J. has received support from CSL Behring. A.L. has received support from CSL Behring. R.M. has received institutional research payments from Abbott, Abiomed, Affluent Medical, Alleviant Medical, Amgen, AM Pharma, Arena, AstraZeneca, AtriCure, Biosensors, Biotronik, Boston Scientific, Bristol Myers Squibb, CardiaWave, CeloNova, CERC, Chiesi, Cleerly Health, Concept Medical, Cytosorbents, Daiichi Sankyo, Duke, Element Science, Essential Medical, Faraday, Idorsia Pharmaceuticals, Janssen, MedAlliance, Mediasphere, Medtelligence, Medtronic, MJH Healthcare, Novartis, OrbusNeich, Penumbra, PhaseBio, Philips, Pi Cardia, PLx Pharma, Population Health Research Institute, Protembis, RecCor Medical, RenalPro, RM Global, Sanofi, Shockwave and Vivasure, Zoll. She received personal fees from Affluent Medical, Boehringer Ingelheim, Cardiovascular Research Foundation (CRF), Cordis, Daiichi Sankyo Brasil, E.R. Squibb Sons, Esperion Science/Innovative Biopharma, Europa Group/Boston Scientific, Gaffney Events, Educational Trust, Henry Ford Health Cardiology, Ionis Pharmaceuticals, Lilly and Company, MedCon International, Novartis, Novo Nordisk, PeerView Institute for Medical Education, TERUMO Europe N.V., Vectura, VoxMedia, WebMD, IQVIA, Radcliffe and TARSUS Cardiology. She received honoraria from the American Medical Association for her role as Associate Editor of
Figures




References
-
- USRDS. 2023 annual data report: epidemiology of kidney disease in the United States. usrds-adr.niddk.nih.gov/2023/introduction (2023). - PubMed
-
- Levey, A. S. et al. Change in albuminuria and GFR as end points for clinical trials in early stages of CKD: a scientific workshop sponsored by the National Kidney Foundation in collaboration with the US Food and Drug Administration and European Medicines Agency. Am. J. Kidney Dis.75, 84–104 (2020). 10.1053/j.ajkd.2019.06.009 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
