

Prognostic clinical decision support for pneumonia in the emergency department: A randomized trial
- PMID: 38797872
- PMCID: PMC11374114
- DOI: 10.1002/jhm.13391
Prognostic clinical decision support for pneumonia in the emergency department: A randomized trial
Abstract
Background: Hospitalization rates for childhood pneumonia vary widely. Risk-based clinical decision support (CDS) interventions may reduce unwarranted variation.
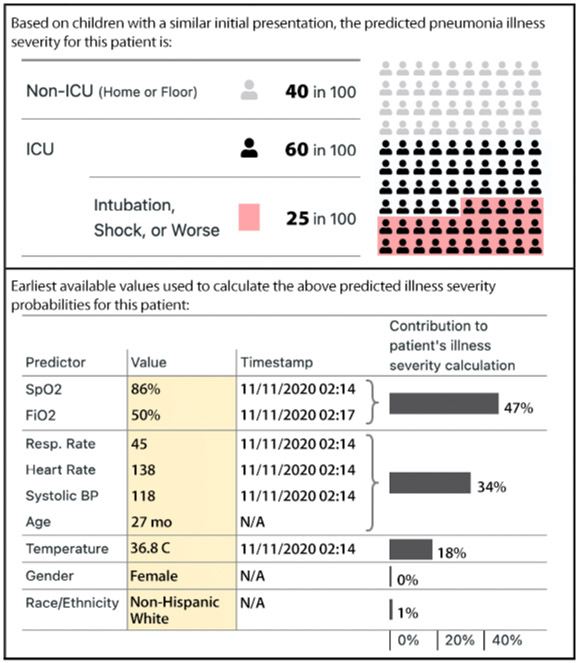
Methods: We conducted a pragmatic randomized trial in two US pediatric emergency departments (EDs) comparing electronic health record (EHR)-integrated prognostic CDS versus usual care for promoting appropriate ED disposition in children (<18 years) with pneumonia. Encounters were randomized 1:1 to usual care versus custom CDS featuring a validated pneumonia severity score predicting risk for severe in-hospital outcomes. Clinicians retained full decision-making authority. The primary outcome was inappropriate ED disposition, defined as early transition to lower- or higher-level care. Safety and implementation outcomes were also evaluated.
Results: The study enrolled 536 encounters (269 usual care and 267 CDS). Baseline characteristics were similar across arms. Inappropriate disposition occurred in 3% of usual care encounters and 2% of CDS encounters (adjusted odds ratio: 0.99, 95% confidence interval: [0.32, 2.95]). Length of stay was also similar and adverse safety outcomes were uncommon in both arms. The tool's custom user interface and content were viewed as strengths by surveyed clinicians (>70% satisfied). Implementation barriers include intrinsic (e.g., reaching the right person at the right time) and extrinsic factors (i.e., global pandemic).
Conclusions: EHR-based prognostic CDS did not improve ED disposition decisions for children with pneumonia. Although the intervention's content was favorably received, low subject accrual and workflow integration problems likely limited effectiveness. Clinical Trials Registration: NCT06033079.
© 2024 Society of Hospital Medicine.
Conflict of interest statement
Figures


References
-
- AHRQ. National Estimates on Use of Hospitals by Children from the HCUP Kids’ Inpatient Database (KID). Published 2012. Accessed January 12, 2014. http://hcupnet.ahrq.gov/
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
