

Imaging findings after a total reconstructed breast with autologous fat transfer: what the radiologist needs to know
- PMID: 38798692
- PMCID: PMC11128096
- DOI: 10.1093/bjro/tzae010
Imaging findings after a total reconstructed breast with autologous fat transfer: what the radiologist needs to know
Abstract
Autologous fat transfer (AFT) is an upcoming technique for total breast reconstruction. Consequently, radiological imaging of women with an AFT reconstructed breast will increase in the coming years, yet radiological experience and evidence after AFT is limited.
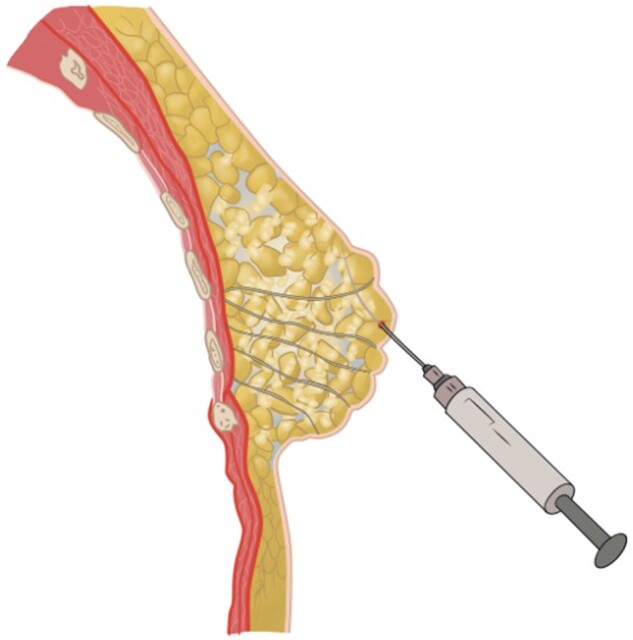
The surgical procedure of AFT and follow-up with imaging modalities including mammography (MG), ultrasound (US), and MRI in patients with a total breast reconstruction with AFT are summarized to illustrate the radiological normal and suspicious findings for malignancy.
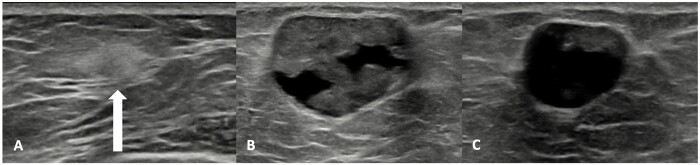
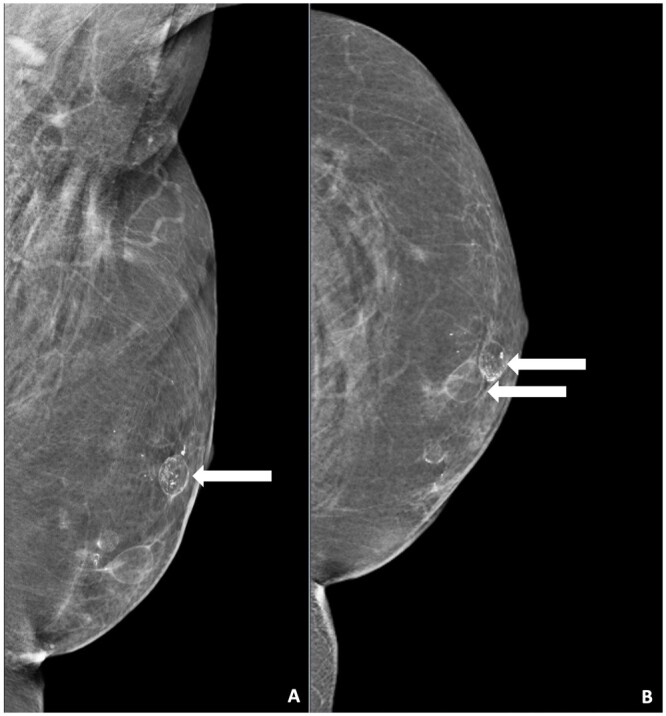
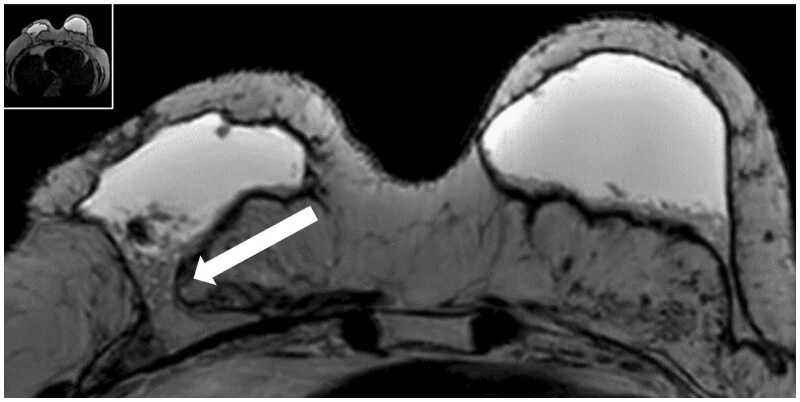
Imaging after a total breast reconstruction with AFT appears to be based mostly on benign imaging findings with an overall low biopsy rate. As higher volumes are injected in this technique, the risk for the onset of fat necrosis increases. Imaging findings most often are related to fat necrosis after AFT. On MG, fat necrosis can mostly be seen as oil cysts. The occurrence of a breast seroma after total breast reconstruction with AFT is an unfavourable outcome and may require special treatment. Fat deposition in the pectoral muscle is a previously unknown, but benign entity. Although fat necrosis is a benign entity, it can mimic breast cancer (recurrence).
In symptomatic women after total breast reconstruction with AFT, MG and US can be considered as first diagnostic modalities. Breast MRI can be used as a problem-solving tool during later stage. Future studies should investigate the most optimal follow-up strategy, including different imaging modalities, in patients treated with AFT for total breast reconstruction.
Keywords: autologous fat transfer (AFT); breast; breast reconstruction; imaging of the reconstructed breast.
© The Author(s) 2024. Published by Oxford University Press on behalf of the British Institute of Radiology.
Conflict of interest statement
None declared.
Figures






References
-
- Zehra S, Doyle F, Barry M, et al.Health-related quality of life following breast reconstruction compared to total mastectomy and breast-conserving surgery among breast cancer survivors: a systematic review and meta-analysis. Breast Cancer. 2020;27(4):534-566. - PubMed
-
- Cordeiro PG. Breast reconstruction after surgery for breast cancer. N Engl J Med. 2008;359(15):1590-1601. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
