

A cost-effectiveness analysis for high versus standard (low) dose caffeine for the treatment of apnea in neonatal intensive care unit
- PMID: 38798766
- PMCID: PMC11123466
- DOI: 10.1080/20523211.2024.2345218
A cost-effectiveness analysis for high versus standard (low) dose caffeine for the treatment of apnea in neonatal intensive care unit
Abstract
Objective: Preterm babies are prone to experiencing apnea of prematurity (AOP), mostly characterised by a pause in breathing lasting a minimum of 20 seconds. Recent literature supported higher maintenance doses of caffeine, indicating benefits. This study evaluated the cost-effectiveness of high maintenance dose (HD) versus low maintenance dose (LD) caffeine for AOP in neonates.
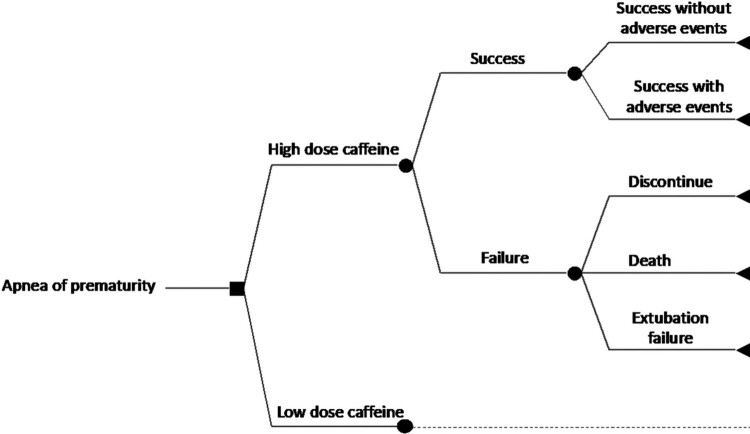
Methods: From the hospital perspective of Hamad Medical Corporation (HMC), Qatar, a cost-effectiveness decision-analytic model was constructed to follow the use of a HD maintenance caffeine of 20 mg/kg/dose versus a LD maintenance caffeine of 10 mg/kg/dose, in a simulated cohort of AOP neonates, over a therapy follow-up duration of six weeks, until neonatal intensive care (NICU) discharge. The clinical inputs were primarily literature-based, while the resource cost and utilisation were locally extracted in HMC. The cost-effectiveness outcome measure was calculated per therapy success, defined as survival with no apnea and successful extubation removal within 72 hours, with or without adverse events. One-way and multivariate sensitivity analyses were performed to confirm the robustness of the results.
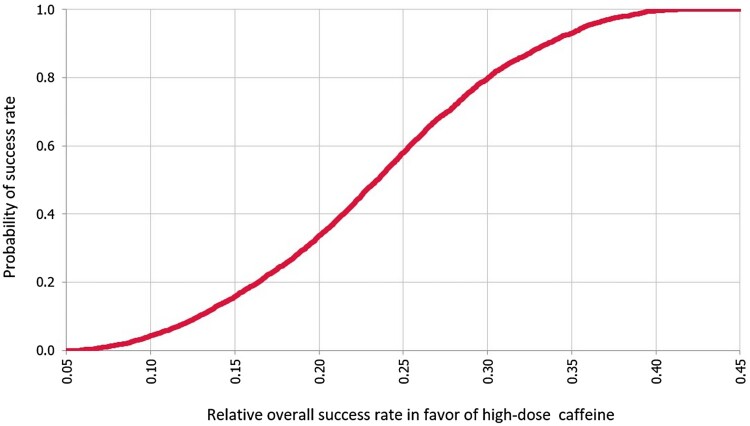
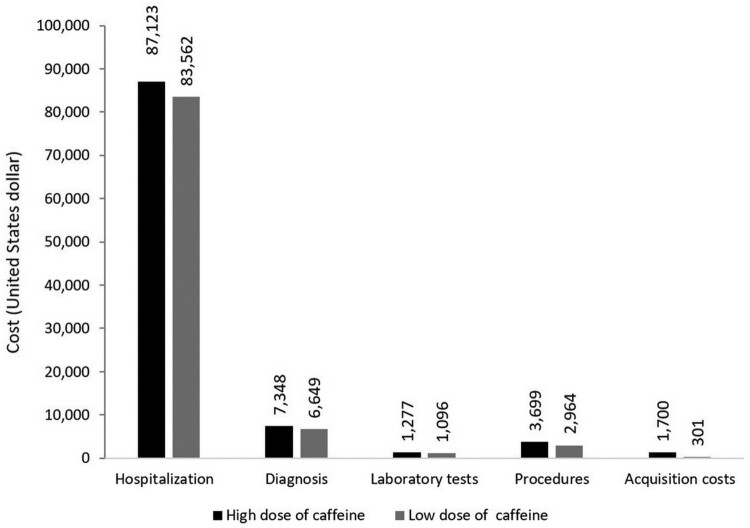
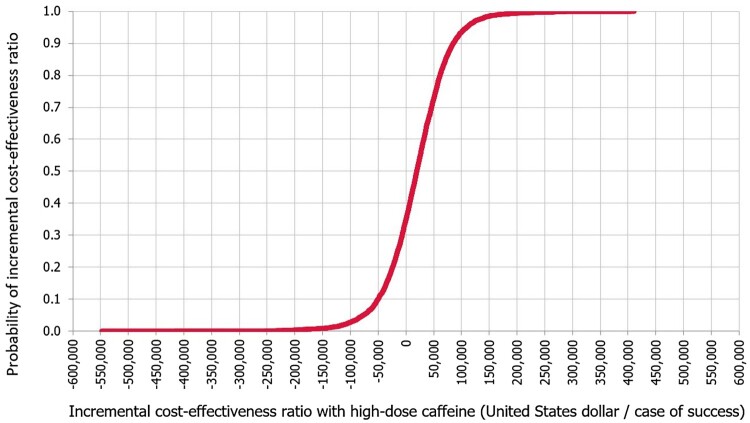
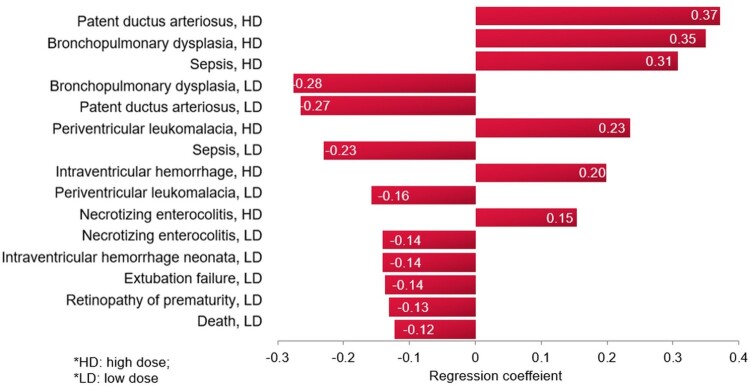
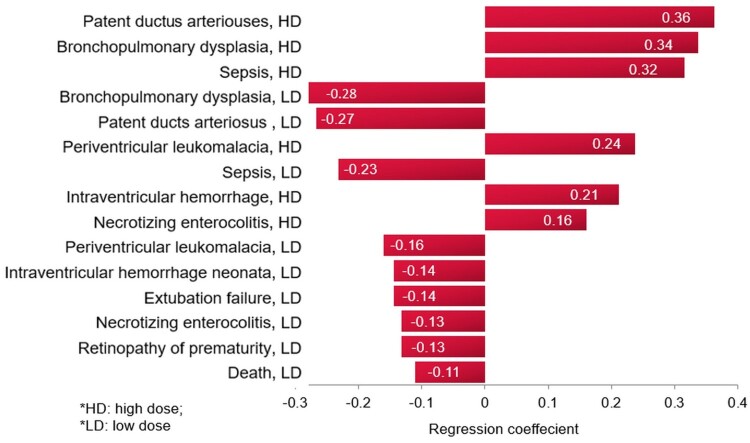
Results: With 0.23 (95% CI, 0.23-0.23) enhancement in success rate, at United States dollar (US$) 3869 (95% CI, US$ 3823-3915) added infant cost, the HD caffeine was between dominant (34.8%) and cost-effective (63.7%), with an average incremental cost-effectiveness ratio of US $16,895 (95% CI, US$ 15,242-18,549) relative to LD caffeine per additional case of success. The hospitalisation contributed the most to the total infant cost, and the probability of patent ductus arteriosus was the model input that influenced the results most.
Conclusion: This is the first literature economic evaluation of caffeine for AOP. Despite increasing the cost of therapy, HD maintenance caffeine seems to be a cost-effective alternative to LD caffeine in Qatar. Our results support the recent global trends of increased use of HD caffeine for AOP in NICU.
Keywords: Cost-effectiveness; apnea; caffeine; intensive care unit; premature infant.
© 2024 The Author(s). Published by Informa UK Limited, trading as Taylor & Francis Group.
Conflict of interest statement
No potential conflict of interest was reported by the author(s).
Figures
Similar articles
-
Caffeine dosing regimens in preterm infants with or at risk for apnea of prematurity.Cochrane Database Syst Rev. 2023 Apr 11;4(4):CD013873. doi: 10.1002/14651858.CD013873.pub2. Cochrane Database Syst Rev. 2023. PMID: 37040532 Free PMC article. Review.
-
Cost-effectiveness of Oral Versus Intravenous Ibuprofen Therapy in Preterm Infants With Patent Ductus Arteriosus in the Neonatal Intensive Care Setting: A Cohort-based Study.Clin Ther. 2021 Feb;43(2):336-348.e7. doi: 10.1016/j.clinthera.2020.12.004. Epub 2021 Jan 9. Clin Ther. 2021. PMID: 33431169
-
Association of Caffeine Daily Dose With Respiratory Outcomes in Preterm Neonates: A Retrospective Cohort Study.Inquiry. 2024 Jan-Dec;61:469580241248098. doi: 10.1177/00469580241248098. Inquiry. 2024. PMID: 38666733 Free PMC article.
-
Clinical and Economic Analysis of Morphine Versus Fentanyl in Managing Ventilated Neonates With Respiratory Distress Syndrome in the Intensive Care Setting.Clin Ther. 2019 Apr;41(4):714-727.e8. doi: 10.1016/j.clinthera.2019.02.009. Epub 2019 Mar 4. Clin Ther. 2019. PMID: 30846286
-
Caffeine: an evidence-based success story in VLBW pharmacotherapy.Pediatr Res. 2018 Sep;84(3):333-340. doi: 10.1038/s41390-018-0089-6. Epub 2018 Jul 9. Pediatr Res. 2018. PMID: 29983414 Review.
Cited by
-
Investigating the effect of oropharyngeal colostrum in the prevention of late-onset sepsis in preterm infants: a randomized controlled trial.Sci Rep. 2025 May 19;15(1):17390. doi: 10.1038/s41598-025-02309-z. Sci Rep. 2025. PMID: 40389508 Free PMC article. Clinical Trial.
References
-
- Abushanab, D., Al-Badriyeh, D., Liew, D., & Ademi, Z. (2022). First-line treatment with empagliflozin and metformin combination versus standard care for patients with type 2 diabetes mellitus and cardiovascular disease in Qatar. A cost-effectiveness analysis. Current Problems in Cardiology, 47(6), 100852. 10.1016/j.cpcardiol.2021.100852. Epub 2021 Apr 6. - DOI - PubMed
-
- Abushanab, D., Rouf, P. A., Al Hail, M., Kamal, R., Viswanathan, B., Parappil, H., Elkassem, W., Al-Shaibi, S., & Al-Badriyeh, D. (2021). Cost-effectiveness of oral versus intravenous ibuprofen therapy in preterm infants with patent ductus arteriosus in the neonatal intensive care setting: A cohort-based study. Clinical Therapeutics, 43(2), 336–348. 10.1016/j.clinthera.2020.12.004 - DOI - PubMed
-
- Al Ansari, E., Qeretli, R., Fayed, M., Altammami, H., Akhras, L., Alalaiyan, S., Alhazzani, F., Binmanee, A., Almidani, E., & Khadawardi, E. (2018). Caffeine therapy practice in the management of apnea of prematurity: National survey in Saudi Arabia. Journal of Clinical Neonatology, 7(4), 217–223. 10.4103/jcn.JCN_45_18 - DOI
-
- Al-Badriyeh, D., Hssain, A. A., & Abushanab, D. (2022). Cost-effectiveness analysis of out-of-hospital versus in-hospital extracorporeal cardiopulmonary resuscitation for out-hospital refractory cardiac arrest. Current Problems in Cardiology, 47(12), 101387. 10.1016/j.cpcardiol.2022.101387. Epub 2022 Sep 5. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials