

Differential risk factor profile and neuroimaging markers of small vessel disease between lacunar ischemic stroke and deep intracerebral hemorrhage
- PMID: 38799702
- PMCID: PMC11119384
- DOI: 10.1177/17562864241253901
Differential risk factor profile and neuroimaging markers of small vessel disease between lacunar ischemic stroke and deep intracerebral hemorrhage
Abstract
Background: Lacunar ischemic stroke (LIS) and deep intracerebral hemorrhage (dICH) are two stroke phenotypes of deep perforator arteriopathy. It is unclear what factors predispose individuals with deep perforator arteriopathy to either ischemic or hemorrhagic events.
Objectives: We aimed to investigate risk factors and neuroimaging features of small vessel disease (SVD) associated with LIS versus dICH in a cross-sectional study.
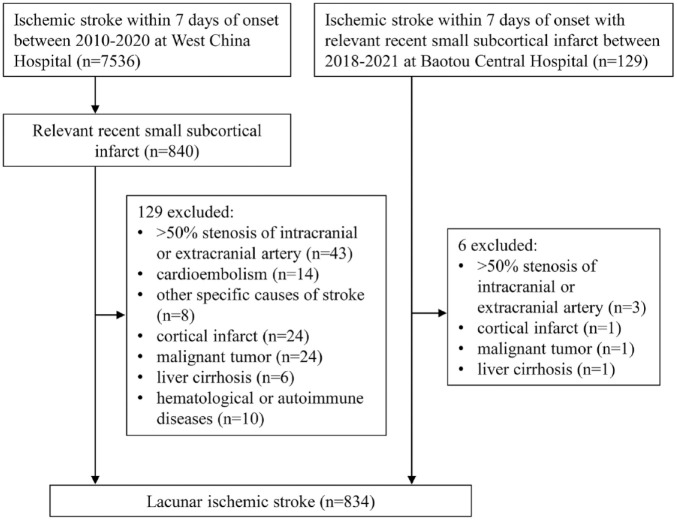
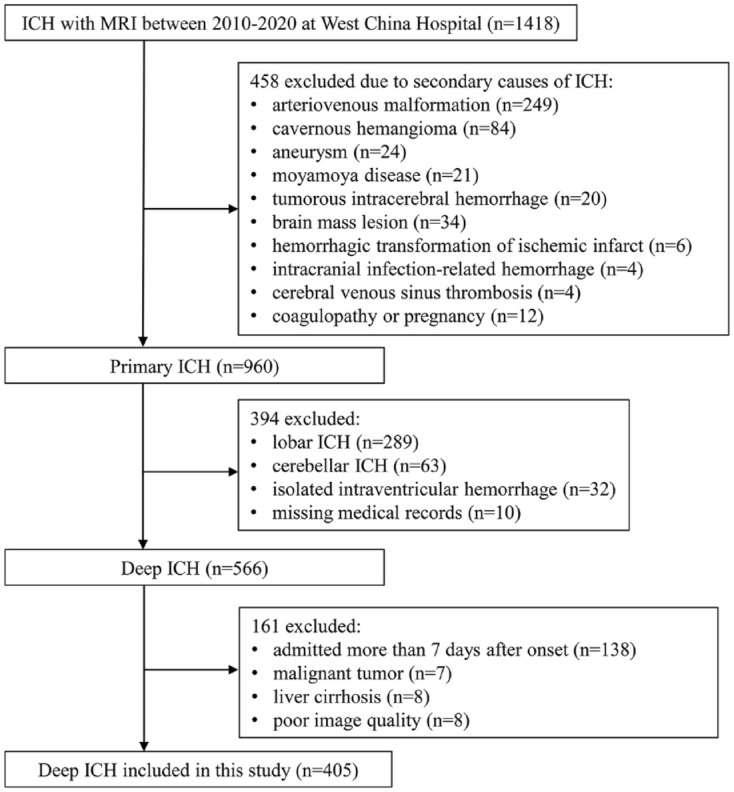
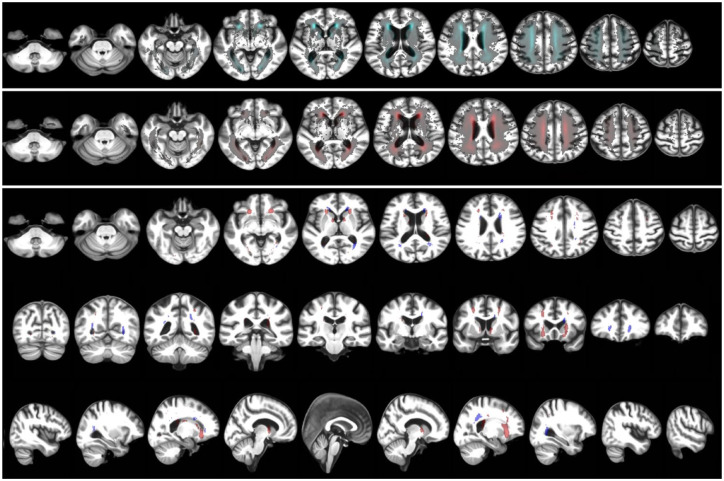
Methods: We included patients with clinically presenting, magnetic resonance imaging-confirmed LIS or dICH from two tertiary hospitals between 2010 and 2021. We recorded vascular risk factors and SVD markers, including lacunes, white matter hyperintensities (WMH), perivascular spaces (PVS), and cerebral microbleeds (CMB). Logistic regression modeling was used to determine the association between vascular risk factors, SVD markers, and stroke phenotype. We further created WMH probability maps to compare WMH distribution between LIS and dICH.
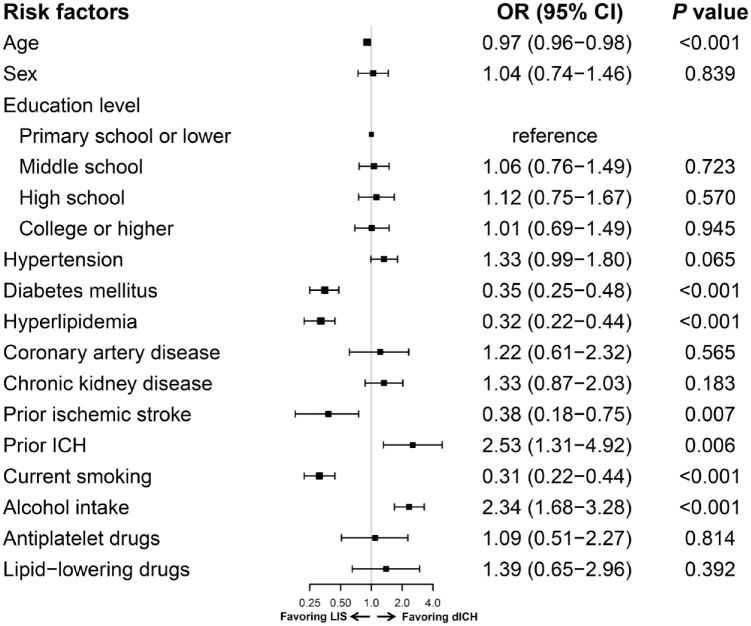
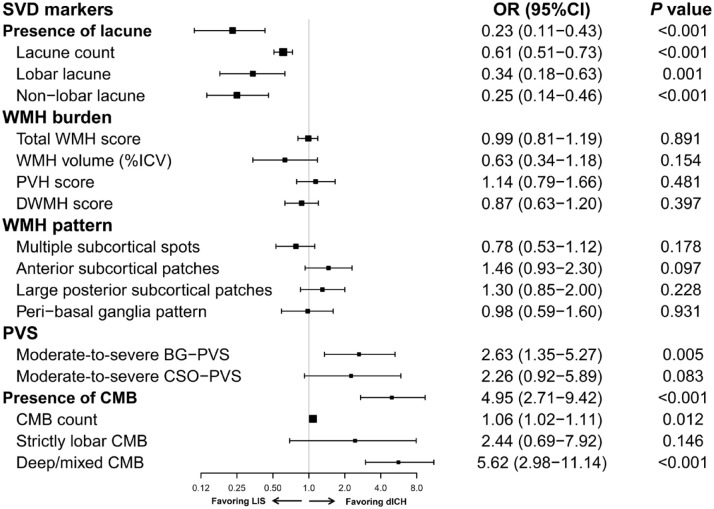
Results: A total of 834 patients with LIS (mean age 61.7 ± 12.1 years) and 405 with dICH (57.7 ± 13.2 years) were included. Hypertension was equally frequent between LIS and dICH (72.3% versus 74.8%, p = 0.349). Diabetes mellitus, hyperlipidemia, smoking, and prior ischemic stroke were more associated with LIS [odds ratio (OR) (95% confidence interval (CI)), 0.35 (0.25-0.48), 0.32 (0.22-0.44), 0.31 (0.22-0.44), and 0.38 (0.18-0.75)]. Alcohol intake and prior ICH were more associated with dICH [OR (95% CI), 2.34 (1.68-3.28), 2.53 (1.31-4.92)]. Lacunes were more prevalent in LIS [OR (95% CI) 0.23 (0.11-0.43)], while moderate-to-severe basal-ganglia PVS and CMB were more prevalent in dICH [OR (95% CI) 2.63 (1.35-5.27), 4.95 (2.71-9.42)]. WMH burden and spatial distribution did not differ between groups.
Conclusion: The microangiopathy underlying LIS and dICH reflects distinct risk profiles and SVD features, hence possibly SVD subtype susceptibility. Prospective studies with careful phenotyping and genetics are needed to clarify the mechanisms underlying this difference.
Keywords: cerebral small vessel disease; deep perforator arteriopathy; intracerebral hemorrhage; lacunar ischemic stroke; risk factor.
© The Author(s), 2024.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Figures
References
-
- van Zagten M, Lodder J, Franke C, et al. Different vascular risk factor profiles in primary intracerebral haemorrhage and small deep infarcts do not suggest similar types of underlying small vessel disease. Cerebrovasc Dis 1994; 4: 121–124.
-
- Janssens E, Mounier-Vehier F, Hamon M, et al. Small subcortical infarcts and primary subcortical haemorrhages may have different risk factors. J Neurol 1995; 242: 425–429. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
