

Latent profile analysis reveals overlapping ARFID and shape/weight motivations for restriction in eating disorders
- PMID: 38801097
- PMCID: PMC11599471
- DOI: 10.1017/S003329172400103X
Latent profile analysis reveals overlapping ARFID and shape/weight motivations for restriction in eating disorders
Abstract
Background: DSM-5 differentiates avoidant/restrictive food intake disorder (ARFID) from other eating disorders (EDs) by a lack of overvaluation of body weight/shape driving restrictive eating. However, clinical observations and research demonstrate ARFID and shape/weight motivations sometimes co-occur. To inform classification, we: (1) derived profiles underlying restriction motivation and examined their validity and (2) described diagnostic characterizations of individuals in each profile to explore whether findings support current diagnostic schemes. We expected, consistent with DSM-5, that profiles would comprise individuals endorsing solely ARFID or restraint (i.e. trying to eat less to control shape/weight) motivations.
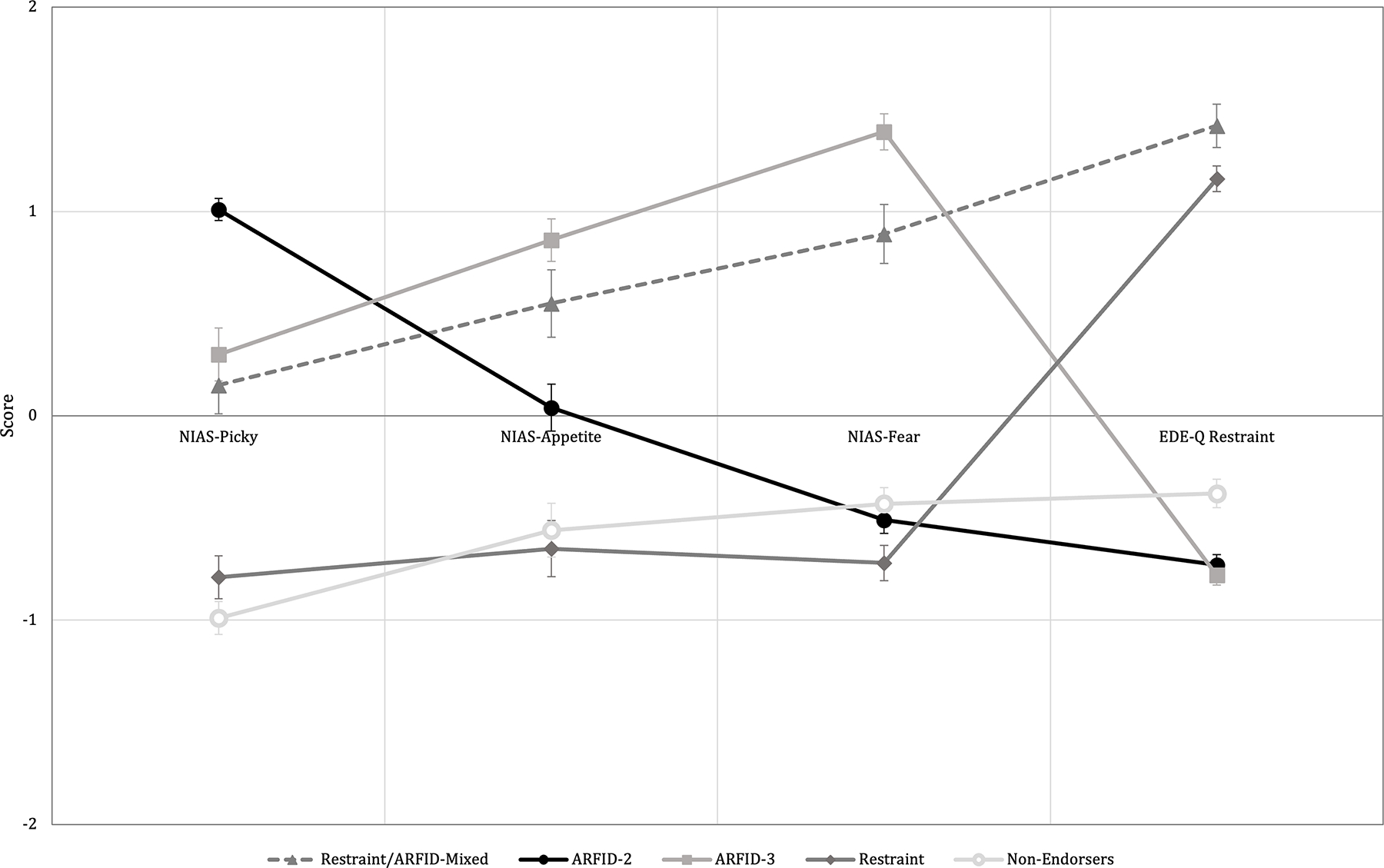
Methods: We applied latent profile analysis to 202 treatment-seeking individuals (ages 10-79 years [M = 26, s.d. = 14], 76% female) with ARFID or a non-ARFID ED, using the Nine-Item ARFID Screen (Picky, Appetite, and Fear subscales) and the Eating Disorder Examination-Questionnaire Restraint subscale as indicators.
Results: A 5-profile solution emerged: Restraint/ARFID-Mixed (n = 24; 8% [n = 2] with ARFID diagnosis); ARFID-2 (with Picky/Appetite; n = 56; 82% ARFID); ARFID-3 (with Picky/Appetite/Fear; n = 40; 68% ARFID); Restraint (n = 45; 11% ARFID); and Non-Endorsers (n = 37; 2% ARFID). Two profiles comprised individuals endorsing solely ARFID motivations (ARFID-2, ARFID-3) and one comprising solely restraint motivations (Restraint), consistent with DSM-5. However, Restraint/ARFID-Mixed (92% non-ARFID ED diagnoses, comprising 18% of those with non-ARFID ED diagnoses in the full sample) endorsed ARFID and restraint motivations.
Conclusions: The heterogeneous profiles identified suggest ARFID and restraint motivations for dietary restriction may overlap somewhat and that individuals with non-ARFID EDs can also endorse high ARFID symptoms. Future research should clarify diagnostic boundaries between ARFID and non-ARFID EDs.
Keywords: anorexia nervosa; avoidant/restrictive food intake disorder; bulimia nervosa.
Conflict of interest statement
Figures
References
-
- Akaike H (1973). Maximum likelihood identification of Gaussian autoregressive moving average models. Biometrika, 60(2), 255–265. doi: 10.1093/biomet/60.2.255 - DOI
-
- Becker KR, Keshishian AC, Liebman RE, Coniglio KA, Wang SB, Franko DL, … & Thomas JJ. (2019). Impact of expanded diagnostic criteria for avoidant/restrictive food intake disorder on clinical comparisons with anorexia nervosa. International Journal of Eating Disorders, 52(3), 230–238. doi: 10.1002/eat.22988 - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
