

The dark side of apnea: altered 24-hour melatonin secretion in obstructive sleep apnea (OSAS) is disease severity dependent
- PMID: 38801480
- PMCID: PMC11303496
- DOI: 10.1007/s11325-024-03066-5
The dark side of apnea: altered 24-hour melatonin secretion in obstructive sleep apnea (OSAS) is disease severity dependent
Abstract
Purpose: Melatonin aids in the synchronization of the circadian rhythm to the external environment. Few studies have tried to elucidate the relationship between melatonin and obstructive sleep apnea syndrome (OSAS). These often include few patients, do not differentiate between OSAS severity and/or do not analyse a 24-h melatonin profile. This study set out to investigate disease severity dependent differences in 24-h salivary melatonin secretion of OSAS patients compared to a reference population in a retrospective design.
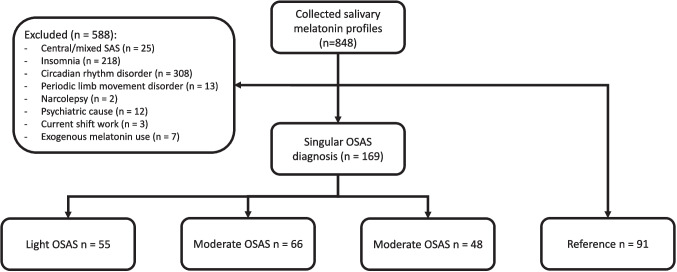
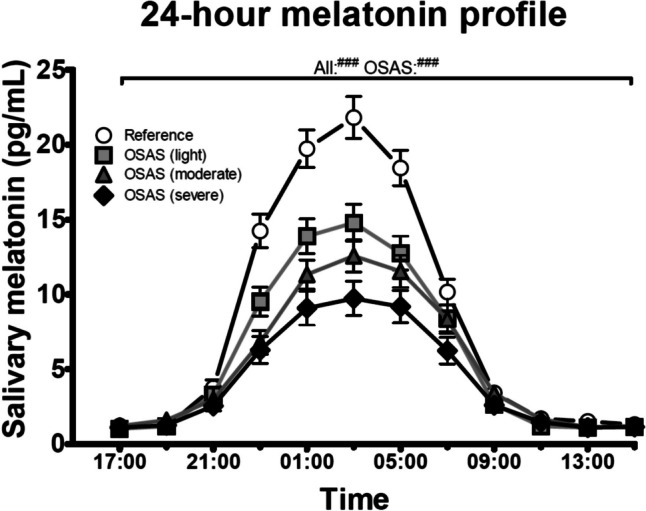
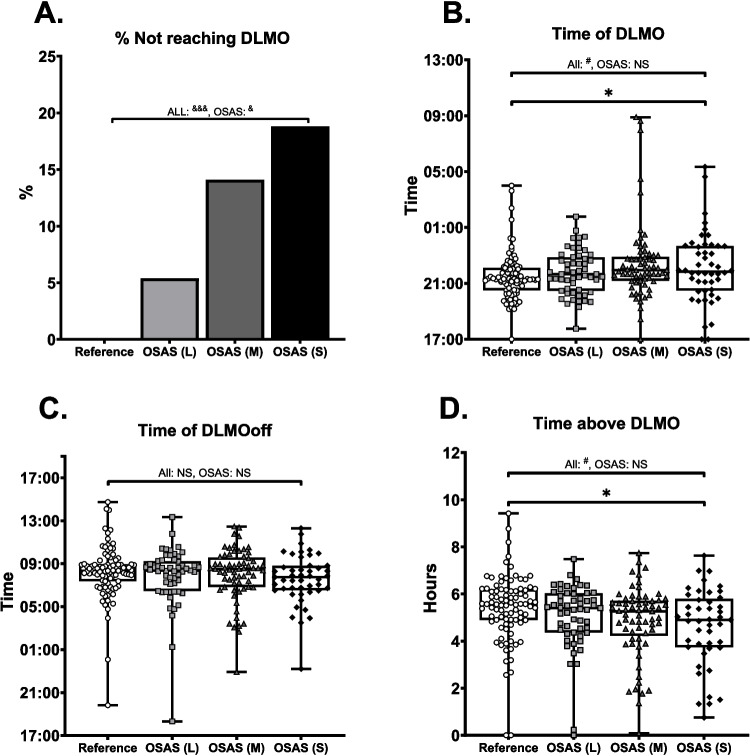
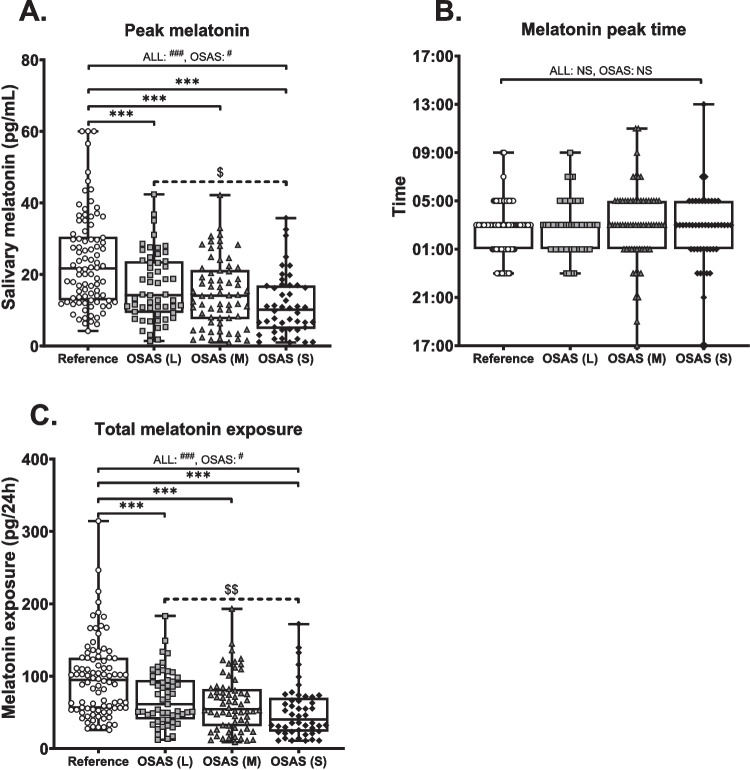
Methods: 24-h salivary melatonin profiles of 169 OSAS patients were analysed (55 light, 66 moderate, 48 severe) as well as 91 reference patients. Several aspects of the melatonin curve were analysed and stratified according to OSAS severity. Parameters included: dim light melatonin onset (DLMO), time of returning below DLMO (DLMOoff), peak melatonin concentration and time, and total melatonin exposure.
Results: Significant effects were corrected for confounding by age and sex using linear regression. Our analysis shows that, compared to reference and in a disease dependent manner, OSAS patients have a significantly lower 24-h melatonin curve, lower melatonin peak concentration, lower total melatonin exposure and a smaller proportion of patients reach DLMO. The differences in peak melatonin production and total melatonin exposure were resistant to confounding by age and/or sex.
Conclusion: This study describes clear OSAS severity dependent abnormalities in melatonin production in OSAS patients, independent of sex and/or age. Future research should indicate whether oral melatonin supplementation has beneficial effects in OSAS patients with attenuated endogenous melatonin production.
Keywords: Circadian rhythm; OSAS; Obstructive sleep apnea; Salivary melatonin.
© 2024. The Author(s).
Conflict of interest statement
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers' bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
Figures
Similar articles
-
Melatonin concentration as a marker of the circadian phase in patients with obstructive sleep apnoea.Sleep Med. 2012 Feb;13(2):167-71. doi: 10.1016/j.sleep.2011.01.020. Epub 2011 Dec 27. Sleep Med. 2012. PMID: 22206710
-
Nocturnal melatonin plasma levels in patients with OSAS: the effect of CPAP.Eur Respir J. 2007 Sep;30(3):496-500. doi: 10.1183/09031936.00051906. Epub 2007 May 30. Eur Respir J. 2007. PMID: 17537771 Clinical Trial.
-
Circadian rhythms in blood pressure, heart rate, hormones, and on polysomnographic parameters in severe obstructive sleep apnea syndrome patients: effect of continuous positive airway pressure.Blood Press Monit. 2016 Jun;21(3):136-43. doi: 10.1097/MBP.0000000000000173. Blood Press Monit. 2016. PMID: 26683380 Clinical Trial.
-
Obstructive sleep apnea syndrome, orexin, and sleep-wake cycle: The link with the neurodegeneration.Handb Clin Neurol. 2025;206:141-160. doi: 10.1016/B978-0-323-90918-1.00014-9. Handb Clin Neurol. 2025. PMID: 39864923 Review.
-
Associations Between Morning Salivary and Blood Cortisol Concentrations in Individuals With Obstructive Sleep Apnea Syndrome: A Meta-Analysis.Front Endocrinol (Lausanne). 2021 Jan 19;11:568823. doi: 10.3389/fendo.2020.568823. eCollection 2020. Front Endocrinol (Lausanne). 2021. PMID: 33542703 Free PMC article.
Cited by
-
Circadian Regulation in Diurnal Mammals: Neural Mechanisms and Implications in Translational Research.Biology (Basel). 2024 Nov 22;13(12):958. doi: 10.3390/biology13120958. Biology (Basel). 2024. PMID: 39765625 Free PMC article. Review.
-
Risk of Major Depression Associated with Excessive Daytime Sleepiness in Apneic Individuals.Clocks Sleep. 2025 Apr 30;7(2):22. doi: 10.3390/clockssleep7020022. Clocks Sleep. 2025. PMID: 40407628 Free PMC article.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
