

A case of immunoglobulin G4-related kidney disease manifesting after dipeptidyl peptidase-4 inhibitor treatment
- PMID: 38801515
- PMCID: PMC11608207
- DOI: 10.1007/s13730-024-00889-9
A case of immunoglobulin G4-related kidney disease manifesting after dipeptidyl peptidase-4 inhibitor treatment
Abstract
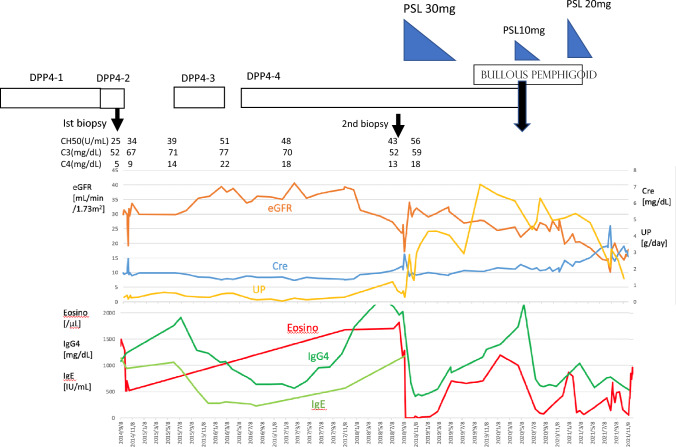
A 68-year-old man with type 2 diabetes mellitus was admitted with decreased renal function. He had high IgG4 (1070 mg/dL) and hypocomplementemia (CH50, 25 U/mL). Kidney biopsy showed tubulointerstitial nephritis with IgG4-positive plasma cell infiltration. Four years later, a second kidney biopsy revealed a new manifestation of membranous nephropathy and tubulointerstitial nephritis with exacerbated fibrosis formation. Six years later, the patient developed bullous pemphigoid, which was thought to be caused by DPP4 inhibitors, so DPP4 inhibitor treatment was discontinued. The use of DPP4 inhibitors correlated with changes in renal function, and the patient was diagnosed with IgG4-related kidney disease related to DPP4 inhibitors.
Keywords: Dipeptidyl peptidase-4 (DPP4) inhibitors; IgG4-related kidney disease; IgG4-related tubulointerstitial nephritis.
© 2024. The Author(s), under exclusive licence to Japanese Society of Nephrology.
Conflict of interest statement
Declarations. Conflicts of interest: The authors declare no competing financial interests and no conflicts of interest. Ethical approval: The present report was produced in conformity with the Declaration of Helsinki, and the patient gave his written informed consent for the case report to be published.
Figures




Similar articles
-
A case of bullous pemphigoid and renal disease after dipeptidyl peptidase 4 inhibitor administration.CEN Case Rep. 2024 Aug;13(4):264-270. doi: 10.1007/s13730-023-00835-1. Epub 2023 Dec 6. CEN Case Rep. 2024. PMID: 38055184 Free PMC article.
-
Low-density lipoprotein apheresis for PLA2R-related membranous glomerulonephritis accompanied by IgG4-related tubulointerstitial nephritis.CEN Case Rep. 2020 Nov;9(4):395-403. doi: 10.1007/s13730-020-00494-6. Epub 2020 Jun 16. CEN Case Rep. 2020. PMID: 32557252 Free PMC article.
-
IgG4-related kidney disease: Clinicopathologic features, differential diagnosis, and mimics.Semin Diagn Pathol. 2024 Mar;41(2):88-94. doi: 10.1053/j.semdp.2023.12.001. Epub 2023 Dec 20. Semin Diagn Pathol. 2024. PMID: 38246802 Review.
-
Role of complement system in patients with biopsy-proven immunoglobulin G4-related kidney disease.Hum Pathol. 2018 Nov;81:220-228. doi: 10.1016/j.humpath.2018.07.008. Epub 2018 Jul 18. Hum Pathol. 2018. PMID: 30031099
-
Renal involvement in IgG4-related disease.Presse Med. 2020 Apr;49(1):104017. doi: 10.1016/j.lpm.2020.104017. Epub 2020 Mar 29. Presse Med. 2020. PMID: 32234380 Review.
Cited by
-
A case of type 2 diabetes mellitus complicated with IgG4-related retroperitoneal fibrosis and a literature review.Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2024 Jul 28;49(7):1073-1081. doi: 10.11817/j.issn.1672-7347.2024.240421. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2024. PMID: 39788495 Free PMC article. Review. Chinese, English.
References
-
- Kawano M, Saeki T, Ubara Y, Matsui S. Recent advances in IgG4-related kidney disease. Mod Rheumatol. 2023;33(2):242–51. - PubMed
-
- Inenaga J, Ueno T, Kawada M, Imafuku A, Mise K, Sumida K, Hiramatsu R, Hasegawa E, Hayami N, Suwabe T, Hoshino J, Sawa N, Takaichi K, Fujii T, Ohashi K, Okaneya T, Ubara Y. IgG4-related disease: a mass lesion in the intrarenal sinus near the renal pelvis. Intern Med. 2015;54(15):1897–900. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
