

Heterogeneity in the definition of major adverse kidney events: a scoping review
- PMID: 38801518
- PMCID: PMC11245451
- DOI: 10.1007/s00134-024-07480-x
Heterogeneity in the definition of major adverse kidney events: a scoping review
Abstract
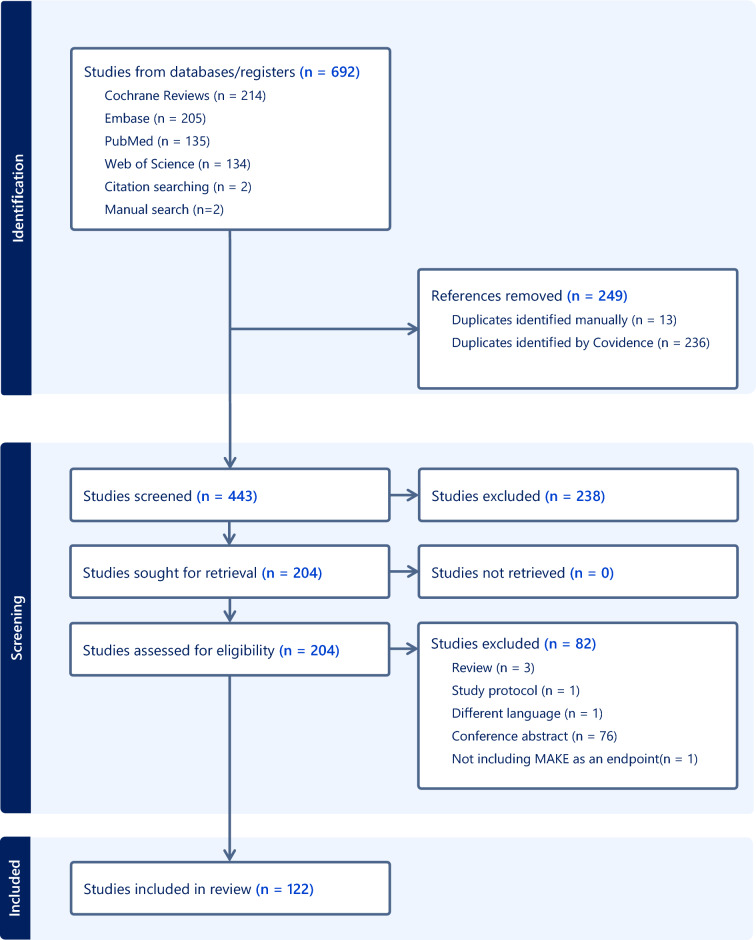
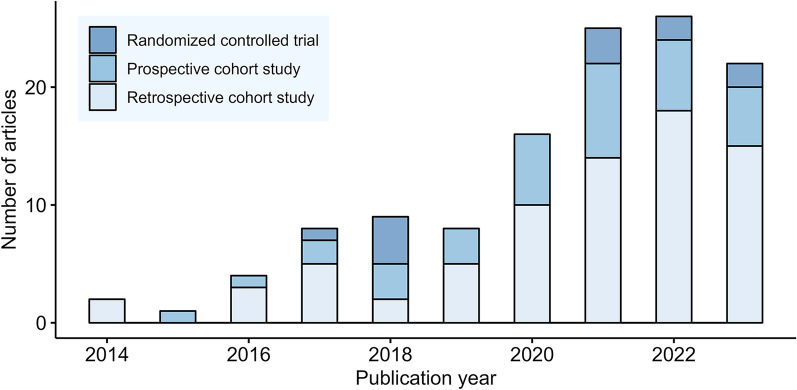
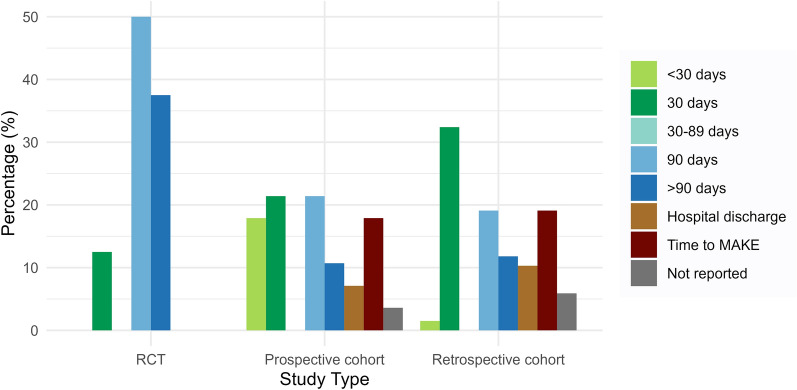
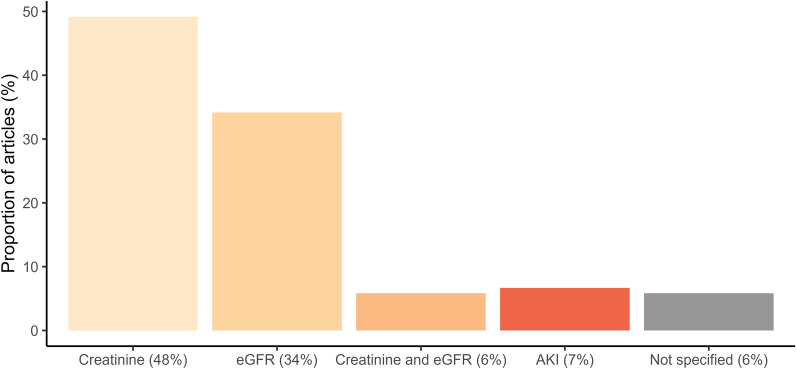
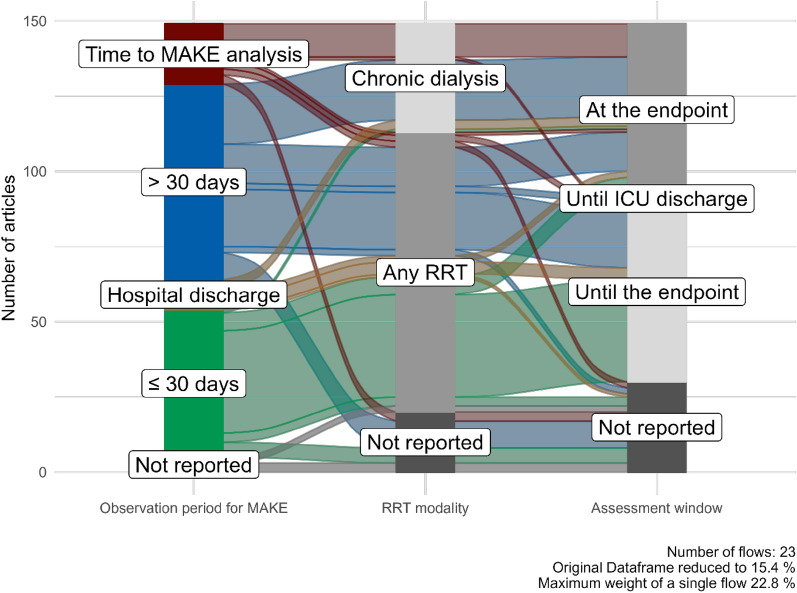
Acute kidney injury (AKI) is associated with persistent renal dysfunction, the receipt of dialysis, dialysis dependence, and mortality. Accordingly, the concept of major adverse kidney events (MAKE) has been adopted as an endpoint for assessing the impact of AKI. However, applied criteria or observation periods for operationalizing MAKE appear to vary across studies. To evaluate this heterogeneity for MAKE evaluation, we performed a systematic scoping review of studies that employed MAKE as an AKI endpoint. Four major academic databases were searched, and we identified 122 studies with increasing numbers over time. We found marked heterogeneity in applied criteria and observation periods for MAKE across these studies, with some even lacking a description of criteria. Moreover, 13 different observation periods were employed, with 30 days and 90 days as the most common. Persistent renal dysfunction was evaluated by estimated glomerular filtration rate (34%) or serum creatinine concentration (48%); however, 37 different definitions for this component were employed in terms of parameters, cut-off criteria, and assessment periods. The definition for the dialysis component also showed significant heterogeneity regarding assessment periods and duration of dialysis requirement (chronic vs temporary). Finally, MAKE rates could vary by 7% [interquartile range: 1.7-16.7%] with different observation periods or by 36.4% with different dialysis component definitions. Our findings revealed marked heterogeneity in MAKE definitions, particularly regarding component assessment and observation periods. Dedicated discussion is needed to establish uniform and acceptable standards to operationalize MAKE in terms of selection and applied criteria of components, observation period, and reporting criteria for future trials on AKI and related conditions.
Keywords: Acute kidney injury; Composite endpoint; Dialysis dependence; Major adverse kidney events.
© 2024. The Author(s).
Conflict of interest statement
There are no financial or any other conflicts of interest, or competing interests associated with this work, writing, and the authors.
Figures
Similar articles
-
Dialysis requirement, long-term major adverse cardiovascular events (MACE) and all-cause mortality in hospital acquired acute kidney injury (AKI): a propensity-matched cohort study.J Nephrol. 2016 Dec;29(6):847-855. doi: 10.1007/s40620-016-0321-6. Epub 2016 Jun 15. J Nephrol. 2016. PMID: 27307250
-
Dialysis Requirement and Long-Term Major Adverse Cardiovascular Events in Patients with Chronic Kidney Disease and Superimposed Acute Kidney Injury.Nephron. 2017;136(2):95-102. doi: 10.1159/000455749. Epub 2017 Mar 2. Nephron. 2017. PMID: 28249270
-
Parameters used to discontinue dialysis in acute kidney injury recovery: a survey of United States nephrologists.Nephron. 2015;130(1):41-7. doi: 10.1159/000381924. Epub 2015 May 19. Nephron. 2015. PMID: 25999063
-
The definitions and staging systems of acute kidney injury and their limitations in practice.Arab J Nephrol Transplant. 2013 Sep;6(3):145-52. Arab J Nephrol Transplant. 2013. PMID: 24053740 Review.
-
Acute Kidney Injury After Liver Transplantation.Transplantation. 2018 Oct;102(10):1636-1649. doi: 10.1097/TP.0000000000002305. Transplantation. 2018. PMID: 29847502
Cited by
-
Fluid balance neutralization secured by hemodynamic monitoring versus protocolized standard of care in patients with acute circulatory failure requiring continuous renal replacement therapy: results of the GO NEUTRAL randomized controlled trial.Intensive Care Med. 2024 Dec;50(12):2061-2072. doi: 10.1007/s00134-024-07676-1. Epub 2024 Oct 17. Intensive Care Med. 2024. PMID: 39417870 Free PMC article. Clinical Trial.
-
Impact of kidney volume on incidence of in-hospital kidney-related adverse outcomes in patients with acute heart failure.BMC Cardiovasc Disord. 2025 Jan 28;25(1):60. doi: 10.1186/s12872-025-04502-4. BMC Cardiovasc Disord. 2025. PMID: 39875830 Free PMC article.
-
Copper-instigated modulatory cell mortality mechanisms and progress in kidney diseases.Ren Fail. 2025 Dec;47(1):2431142. doi: 10.1080/0886022X.2024.2431142. Epub 2025 Jan 13. Ren Fail. 2025. PMID: 39805816 Free PMC article. Review.
-
A phase 3 study of ravulizumab to protect patients with chronic kidney disease from cardiac surgery-associated acute kidney injury and major adverse kidney events (ARTEMIS).Trials. 2025 May 30;26(1):181. doi: 10.1186/s13063-025-08895-7. Trials. 2025. PMID: 40448185 Free PMC article.
-
Epidemiology and long-term outcomes of critically ill patients with severe AKI in India and Southeast Asia.Intensive Care Med. 2025 Jul;51(7):1306-1319. doi: 10.1007/s00134-025-08008-7. Epub 2025 Jul 14. Intensive Care Med. 2025. PMID: 40658243
References
-
- Hoste EA, Bagshaw SM, Bellomo R, Cely CM, Colman R, Cruz DN, Edipidis K, Forni LG, Gomersall CD, Govil D, Honore PM, Joannes-Boyau O, Joannidis M, Korhonen AM, Lavrentieva A, Mehta RL, Palevsky P, Roessler E, Ronco C, Uchino S, Vazquez JA, Vidal Andrade E, Webb S, Kellum JA. Epidemiology of acute kidney injury in critically ill patients: the multinational AKI-EPI study. Intensive Care Med. 2015;41:1411–1423. doi: 10.1007/s00134-015-3934-7. - DOI - PubMed
-
- See EJ, Jayasinghe K, Glassford N, Bailey M, Johnson DW, Polkinghorne KR, Toussaint ND, Bellomo R. Long-term risk of adverse outcomes after acute kidney injury: a systematic review and meta-analysis of cohort studies using consensus definitions of exposure. Kidney Int. 2019;95:160–172. doi: 10.1016/j.kint.2018.08.036. - DOI - PubMed
-
- Kellum J, Lameire N, Aspelin P. KDIGO clinical practice guideline for acute kidney injury. Kidney Int Suppl. 2012;2:1–138. doi: 10.1038/kisup.2012.1. - DOI
-
- Chawla LS, Bellomo R, Bihorac A, Goldstein SL, Siew ED, Bagshaw SM, Bittleman D, Cruz D, Endre Z, Fitzgerald RL, Forni L, Kane-Gill SL, Hoste E, Koyner J, Liu KD, Macedo E, Mehta R, Murray P, Nadim M, Ostermann M, Palevsky PM, Pannu N, Rosner M, Wald R, Zarbock A, Ronco C, Kellum JA, Acute Disease Quality Initiative W Acute kidney disease and renal recovery: consensus report of the Acute Disease Quality Initiative (ADQI) 16 Workgroup. Nat Rev Nephrol. 2017;13:241–257. doi: 10.1038/nrneph.2017.2. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
