

Exploring the lung-gut direction of the gut-lung axis in patients with ARDS
- PMID: 38802959
- PMCID: PMC11131229
- DOI: 10.1186/s13054-024-04966-4
Exploring the lung-gut direction of the gut-lung axis in patients with ARDS
Abstract
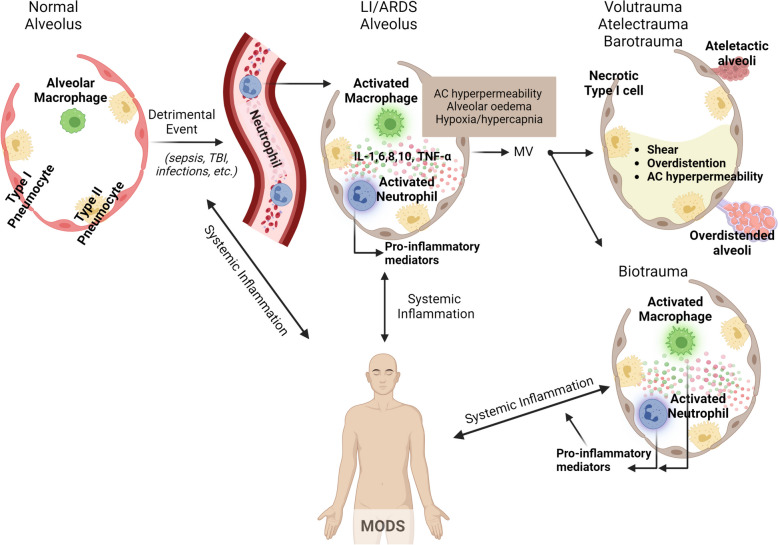
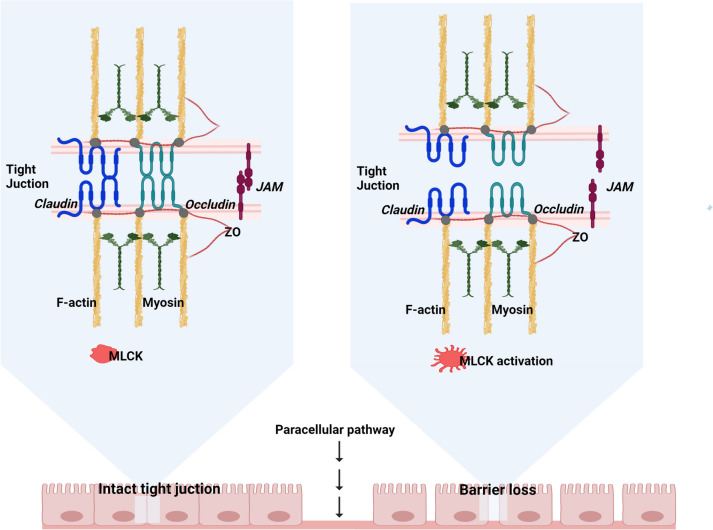
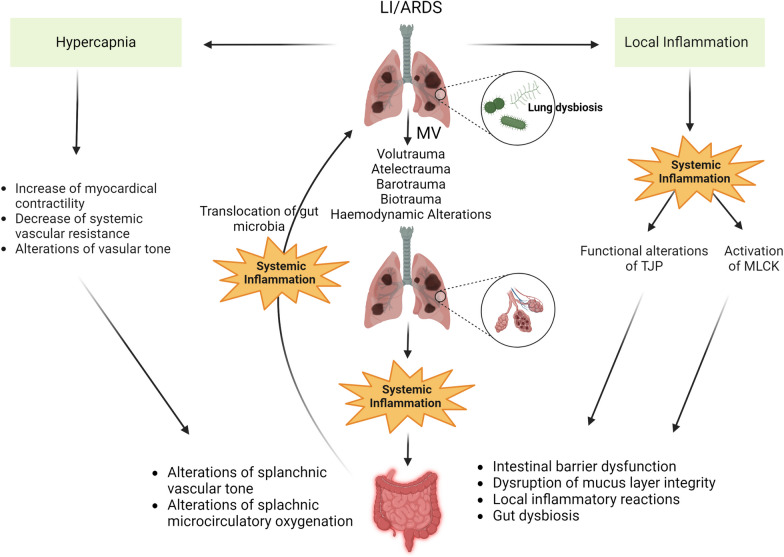
Acute respiratory distress syndrome (ARDS) represents a life-threatening inflammatory reaction marked by refractory hypoxaemia and pulmonary oedema. Despite advancements in treatment perspectives, ARDS still carries a high mortality rate, often due to systemic inflammatory responses leading to multiple organ dysfunction syndrome (MODS). Indeed, the deterioration and associated mortality in patients with acute lung injury (LI)/ARDS is believed to originate alongside respiratory failure mainly from the involvement of extrapulmonary organs, a consequence of the complex interaction between initial inflammatory cascades related to the primary event and ongoing mechanical ventilation-induced injury resulting in multiple organ failure (MOF) and potentially death. Even though recent research has increasingly highlighted the role of the gastrointestinal tract in this process, the pathophysiology of gut dysfunction in patients with ARDS remains mainly underexplored. This review aims to elucidate the complex interplay between lung and gut in patients with LI/ARDS. We will examine various factors, including systemic inflammation, epithelial barrier dysfunction, the effects of mechanical ventilation (MV), hypercapnia, and gut dysbiosis. Understanding these factors and their interaction may provide valuable insights into the pathophysiology of ARDS and potential therapeutic strategies to improve patient outcomes.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Role of gut microbes in acute lung injury/acute respiratory distress syndrome.Gut Microbes. 2024 Jan-Dec;16(1):2440125. doi: 10.1080/19490976.2024.2440125. Epub 2024 Dec 10. Gut Microbes. 2024. PMID: 39658851 Free PMC article. Review.
-
Pathophysiological mechanisms of ARDS: a narrative review from molecular to organ-level perspectives.Respir Res. 2025 Feb 13;26(1):54. doi: 10.1186/s12931-025-03137-5. Respir Res. 2025. PMID: 39948645 Free PMC article. Review.
-
Acute respiratory distress syndrome.Lancet. 2021 Aug 14;398(10300):622-637. doi: 10.1016/S0140-6736(21)00439-6. Epub 2021 Jul 1. Lancet. 2021. PMID: 34217425 Free PMC article. Review.
-
Gut-derived immune cells and the gut-lung axis in ARDS.Crit Care. 2024 Jul 4;28(1):220. doi: 10.1186/s13054-024-05006-x. Crit Care. 2024. PMID: 38965622 Free PMC article. Review.
-
Acute lung injury - from pathophysiology to treatment.Physiol Res. 2020 Dec 31;69(Suppl 3):S353-S366. doi: 10.33549/physiolres.934602. Physiol Res. 2020. PMID: 33464919 Free PMC article. Review.
Cited by
-
Gut microbiota characteristics in neonatal respiratory distress syndrome and the therapeutic potential of probiotics in recovery.Front Microbiol. 2025 Apr 4;16:1544055. doi: 10.3389/fmicb.2025.1544055. eCollection 2025. Front Microbiol. 2025. PMID: 40256622 Free PMC article.
-
Deciphering and steering population-level response under spatial drug heterogeneity on microhabitat structures.bioRxiv [Preprint]. 2025 Jun 17:2025.02.13.638200. doi: 10.1101/2025.02.13.638200. bioRxiv. 2025. PMID: 40027692 Free PMC article. Preprint.
-
Fluid management strategies in critically ill patients with ARDS: a narrative review.Eur J Med Res. 2025 May 20;30(1):401. doi: 10.1186/s40001-025-02661-w. Eur J Med Res. 2025. PMID: 40394685 Free PMC article. Review.
-
Impact of fecal microbiota transplantation on lung function and gut microbiome in an ARDS rat model: A multi-omics analysis including 16S rRNA sequencing, metabolomics, and transcriptomics.Int J Immunopathol Pharmacol. 2025 Jan-Dec;39:3946320251333982. doi: 10.1177/03946320251333982. Epub 2025 Apr 23. Int J Immunopathol Pharmacol. 2025. PMID: 40265594 Free PMC article.
-
Personalized Nutrition in the Pediatric ICU: Steering the Shift from Acute Stress to Metabolic Recovery and Rehabilitation.Nutrients. 2024 Oct 17;16(20):3523. doi: 10.3390/nu16203523. Nutrients. 2024. PMID: 39458517 Free PMC article. Review.
References
-
- Force ADT, et al. Acute respiratory distress syndrome: the Berlin definition. JAMA. 2012;307(23):2526–2533. - PubMed
