

Diagnostic yield and clinical impact of germline sequencing in children with CNS and extracranial solid tumors-a nationwide, prospective Swedish study
- PMID: 38803632
- PMCID: PMC11129334
- DOI: 10.1016/j.lanepe.2024.100881
Diagnostic yield and clinical impact of germline sequencing in children with CNS and extracranial solid tumors-a nationwide, prospective Swedish study
Abstract
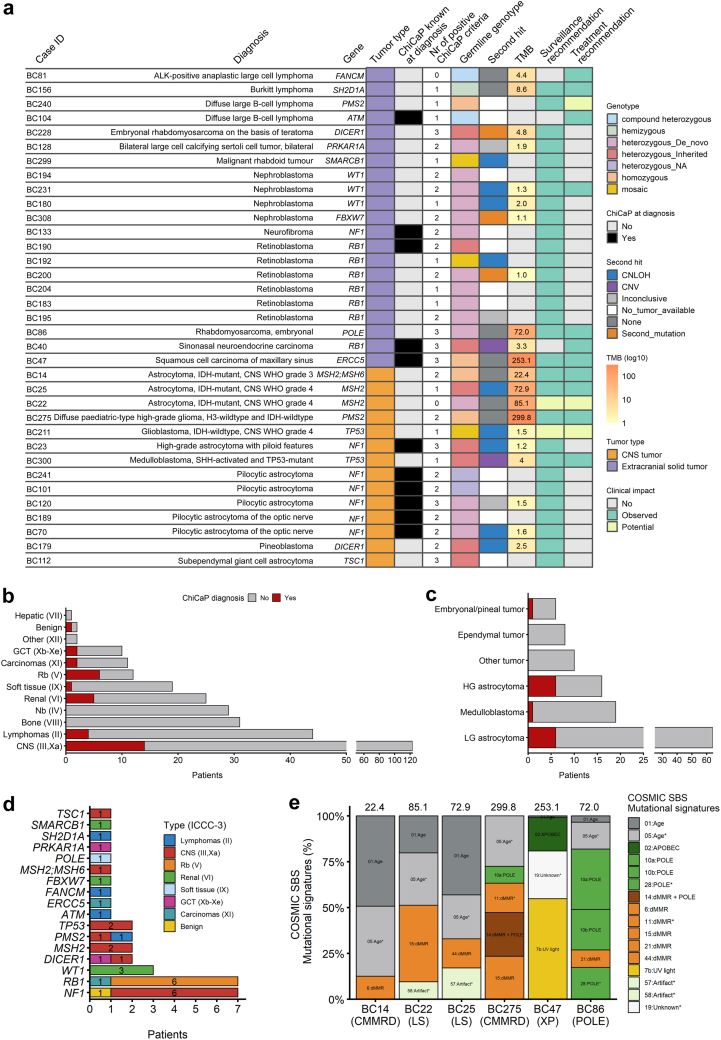
Background: Childhood cancer predisposition (ChiCaP) syndromes are increasingly recognized as contributing factors to childhood cancer development. Yet, due to variable availability of germline testing, many children with ChiCaP might go undetected today. We report results from the nationwide and prospective ChiCaP study that investigated diagnostic yield and clinical impact of integrating germline whole-genome sequencing (gWGS) with tumor sequencing and systematic phenotyping in children with solid tumors.
Methods: gWGS was performed in 309 children at diagnosis of CNS (n = 123, 40%) or extracranial (n = 186, 60%) solid tumors and analyzed for disease-causing variants in 189 known cancer predisposing genes. Tumor sequencing data were available for 74% (227/309) of patients. In addition, a standardized clinical assessment for underlying predisposition was performed in 95% (293/309) of patients.
Findings: The prevalence of ChiCaP diagnoses was 11% (35/309), of which 69% (24/35) were unknown at inclusion (diagnostic yield 8%, 24/298). A second-hit and/or relevant mutational signature was observed in 19/21 (90%) tumors with informative data. ChiCaP diagnoses were more prevalent among patients with retinoblastomas (50%, 6/12) and high-grade astrocytomas (37%, 6/16), and in those with non-cancer related features (23%, 20/88), and ≥2 positive ChiCaP criteria (28%, 22/79). ChiCaP diagnoses were autosomal dominant in 80% (28/35) of patients, yet confirmed de novo in 64% (18/28). The 35 ChiCaP findings resulted in tailored surveillance (86%, 30/35) and treatment recommendations (31%, 11/35).
Interpretation: Overall, our results demonstrate that systematic phenotyping, combined with genomics-based diagnostics of ChiCaP in children with solid tumors is feasible in large-scale clinical practice and critically guides personalized care in a sizable proportion of patients.
Funding: The study was supported by the Swedish Childhood Cancer Fund and the Ministry of Health and Social Affairs.
Keywords: Childhood cancer predisposition; Germline variants; Somatic mutations; Whole-genome sequencing.
© 2024 The Author(s).
Conflict of interest statement
BT, FA, ET, and AN received support from the Swedish Childhood Cancer Fund (BT: TJ2018-0042; FA: KP2021-0010; ET: TJ2021-0125; AN: KP2019-0024, PR2019-0027, TJ2019-0013) and the Swedish Cancer Fund (FA: 21 1540 Fk 01 H; ET: 22 2451Fk; AN: 22 2057Pj). BT, ET and AN received support from Region Stockholm (BT: FoUI-985957; ET: FoUI-973659; AN: 5010124 ALF, 520136 ALF). AN received support from The Swedish Research Council (2021-02860). MB received honoraria for lectures by the Swedish Childhood Cancer Fund. GS served as advisor for trial design for Cyxone AB, Sweden. NH served as Chair of NOPHO Scientific Committee and Young NOPHO without retribution. RR received honoraria from AbbVie, AstraZeneca, Janssen, Illumina, and Roche. DG received grants from Swedish Ministry of Health and Social Affairs for GMS Childhood Cancer and is Vice dean for internationalization and recruitment, Faculty of Medicine, Lund University. AN received also funding from the Cancer Society of Stockholm, Stiftelsen Frimurare Barnhuset i Stockholm, Hållsten research foundation, Berth von Kantzow foundation and is board member of Sävstaholm foundation, Ågrenska foundation, Sällsyntafonden. All other authors have no conflict of interest to declare.
Figures


References
-
- Swedish childhood cancer registry annual report, Barncancerregistret. 2021. https://sbcr.se/ Available from:
-
- Kratz C.P., Jongmans M.C., Cavé H., et al. Predisposition to cancer in children and adolescents. Lancet Child Adolesc Health. 2021;5(2):142–154. - PubMed
-
- Wong M., Mayoh C., Lau L.M.S., et al. Whole genome, transcriptome and methylome profiling enhances actionable target discovery in high-risk pediatric cancer. Nat Med. 2020;26(11):1742–1753. - PubMed
LinkOut - more resources
Full Text Sources
