

Acute myocardial infarction prognosis prediction with reliable and interpretable artificial intelligence system
- PMID: 38804963
- PMCID: PMC11187491
- DOI: 10.1093/jamia/ocae114
Acute myocardial infarction prognosis prediction with reliable and interpretable artificial intelligence system
Abstract
Objective: Predicting mortality after acute myocardial infarction (AMI) is crucial for timely prescription and treatment of AMI patients, but there are no appropriate AI systems for clinicians. Our primary goal is to develop a reliable and interpretable AI system and provide some valuable insights regarding short, and long-term mortality.
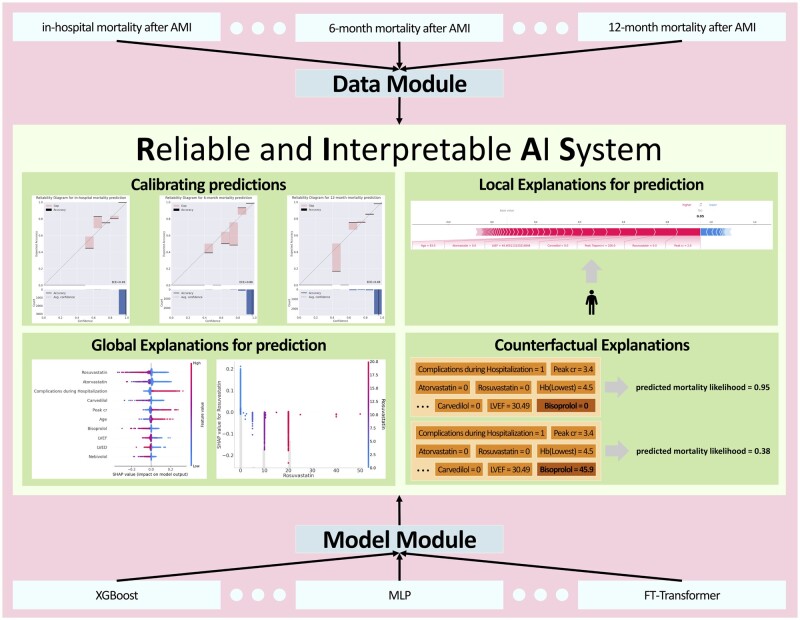
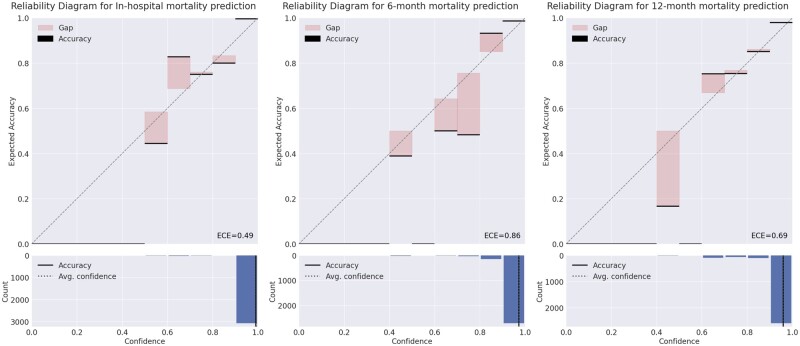
Materials and methods: We propose the RIAS framework, an end-to-end framework that is designed with reliability and interpretability at its core and automatically optimizes the given model. Using RIAS, clinicians get accurate and reliable predictions which can be used as likelihood, with global and local explanations, and "what if" scenarios to achieve desired outcomes as well.
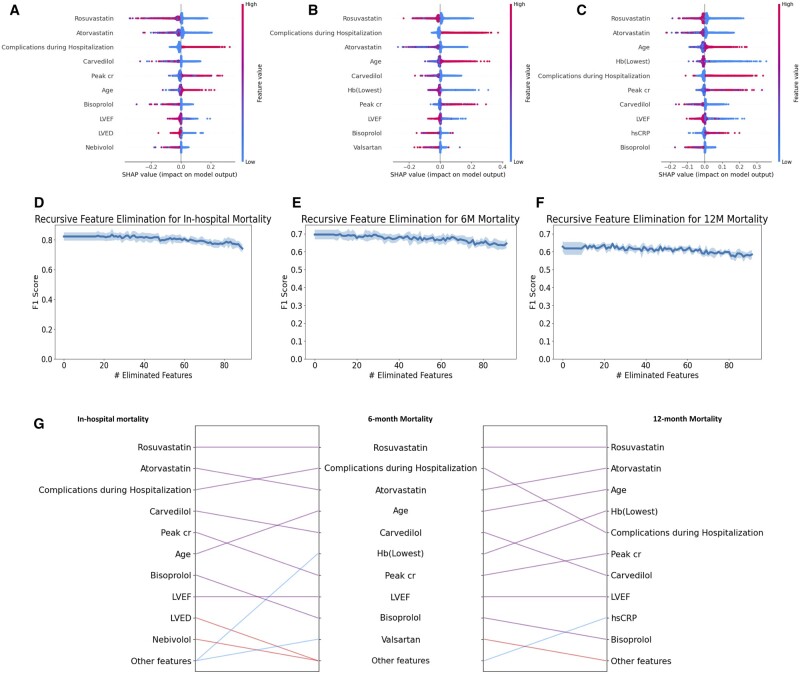
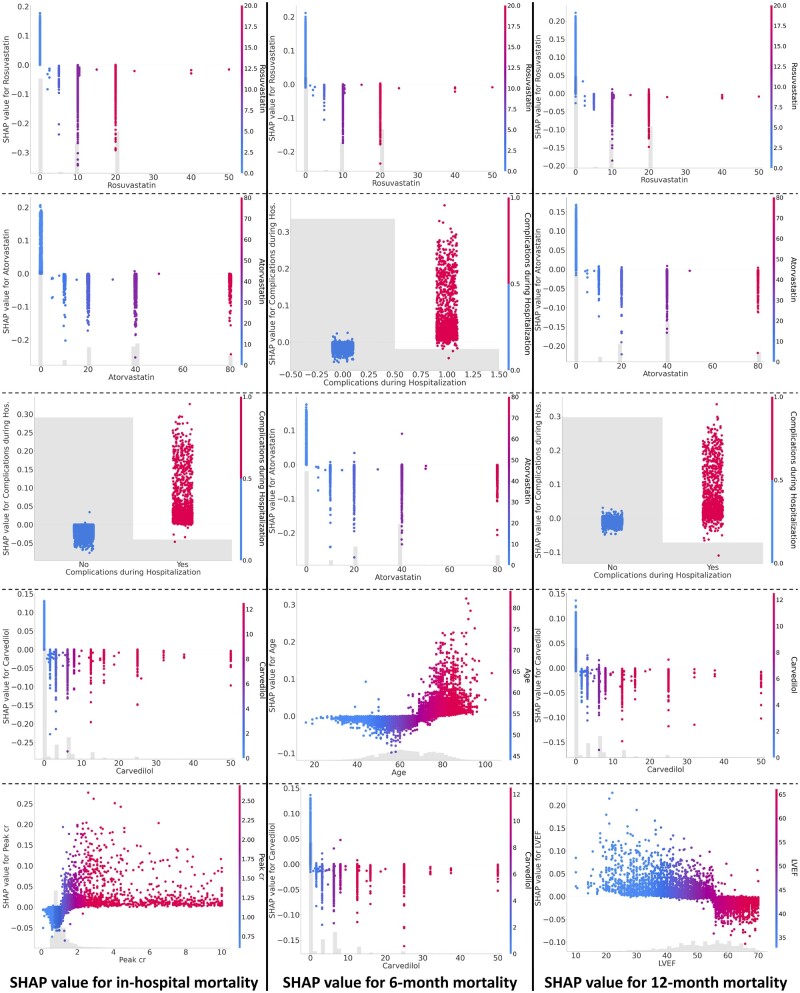
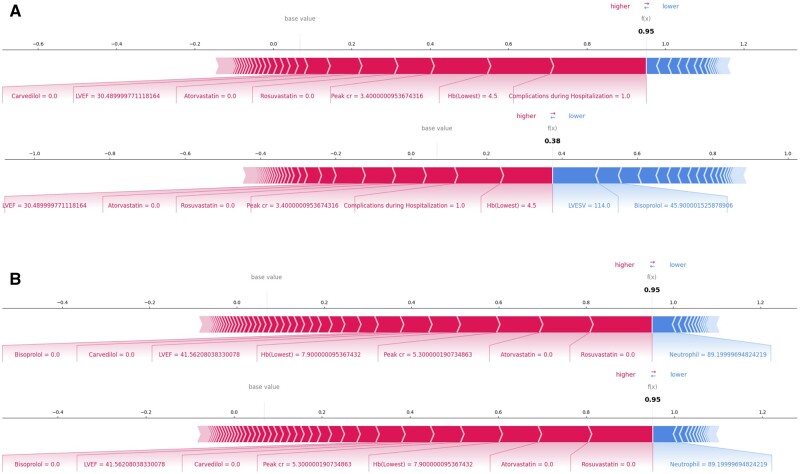
Results: We apply RIAS to AMI prognosis prediction data which comes from the Korean Acute Myocardial Infarction Registry. We compared FT-Transformer with XGBoost and MLP and found that FT-Transformer has superiority in sensitivity and comparable performance in AUROC and F1 score to XGBoost. Furthermore, RIAS reveals the significance of statin-based medications, beta-blockers, and age on mortality regardless of time period. Lastly, we showcase reliable and interpretable results of RIAS with local explanations and counterfactual examples for several realistic scenarios.
Discussion: RIAS addresses the "black-box" issue in AI by providing both global and local explanations based on SHAP values and reliable predictions, interpretable as actual likelihoods. The system's "what if" counterfactual explanations enable clinicians to simulate patient-specific scenarios under various conditions, enhancing its practical utility.
Conclusion: The proposed framework provides reliable and interpretable predictions along with counterfactual examples.
Keywords: acute myocardial infarction; counterfactual explanation; electronic health records (EHR); explainable artificial intelligence (XAI); interpretable machine learning.
© The Author(s) 2024. Published by Oxford University Press on behalf of the American Medical Informatics Association.
Conflict of interest statement
None declared.
Figures
References
-
- Tsao CW, Aday AW, Almarzooq ZI, et al. ; American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2023 update: a report from the American Heart Association. Circulation. 2023;147(8):e93-e621. - PMC - PubMed
-
- Antman EM, Cohen M, Bernink PJLM, et al. The TIMI risk score for unstable angina/non-ST elevation MI: a method for prognostication and therapeutic decision making. JAMA. 2000;284(7):835-842. - PubMed
-
- Morrow DA, Antman EM, Charlesworth A, et al. TIMI risk score for ST-elevation myocardial infarction: a convenient, bedside. clinical score for risk assessment at presentation: an intravenous nPA for treatment of infarcting myocardium early II trial substudy. Circulation. 2000;102(17):2031-2037. - PubMed
-
- Abu-Assi E, Garćıa-Acũna JM, Peña-Gil C, et al. Validation of the GRACE risk score for predicting death within 6 months of follow-up in a contemporary cohort of patients with acute coronary syndrome. Rev Esp Cardiol. 2010;63(6):640-648. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
