

Barriers to engagement in the care cascade for tuberculosis disease in India: A systematic review of quantitative studies
- PMID: 38805509
- PMCID: PMC11166313
- DOI: 10.1371/journal.pmed.1004409
Barriers to engagement in the care cascade for tuberculosis disease in India: A systematic review of quantitative studies
Abstract
Background: India accounts for about one-quarter of people contracting tuberculosis (TB) disease annually and nearly one-third of TB deaths globally. Many Indians do not navigate all care cascade stages to receive TB treatment and achieve recurrence-free survival. Guided by a population/exposure/comparison/outcomes (PECO) framework, we report findings of a systematic review to identify factors contributing to unfavorable outcomes across each care cascade gap for TB disease in India.
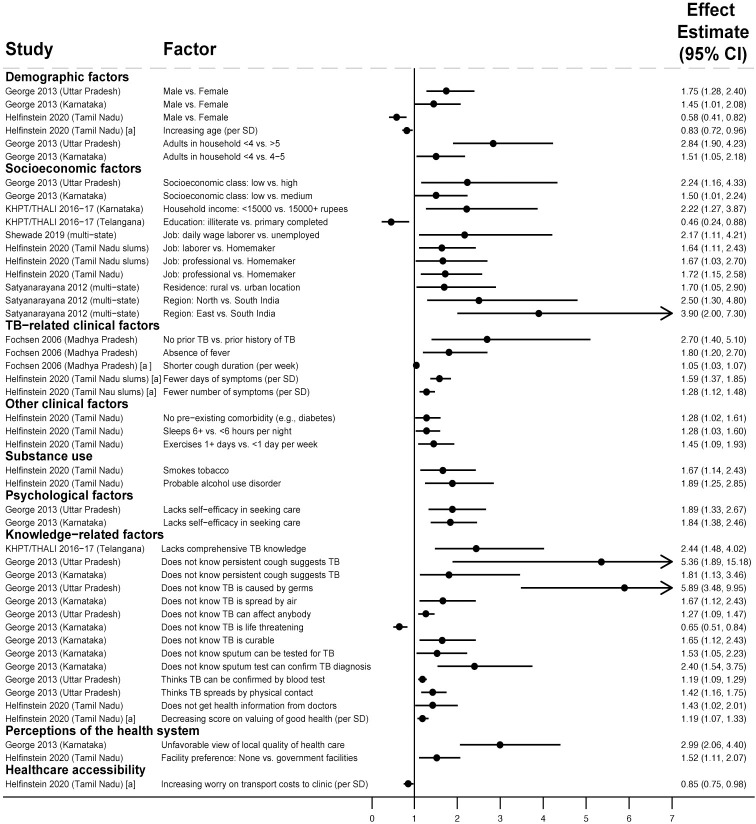
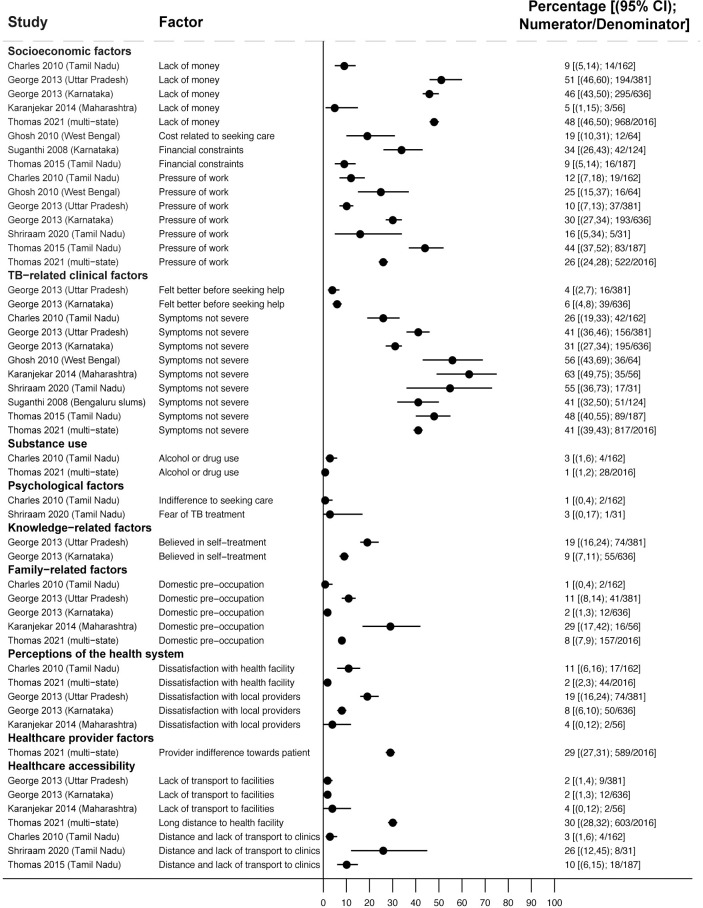
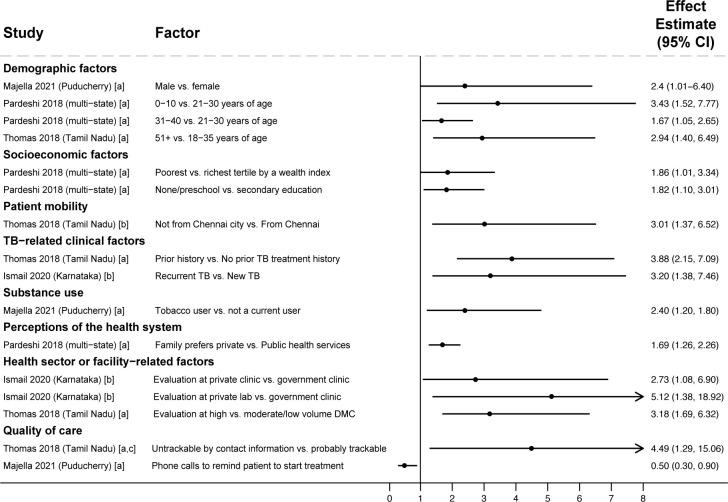
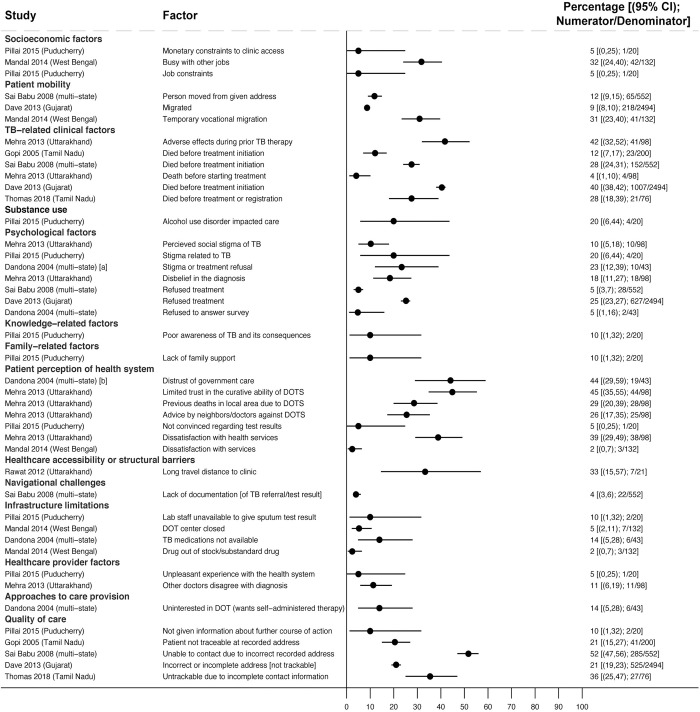
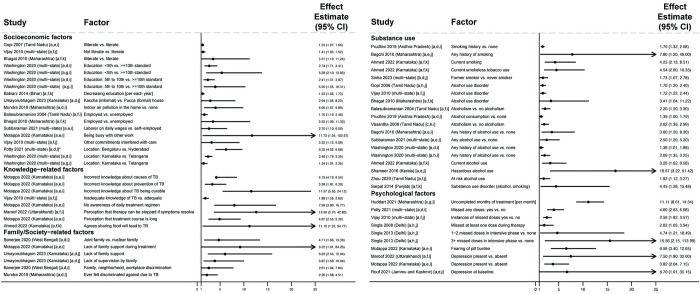
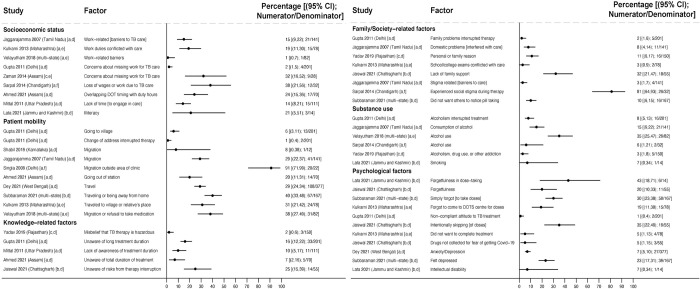
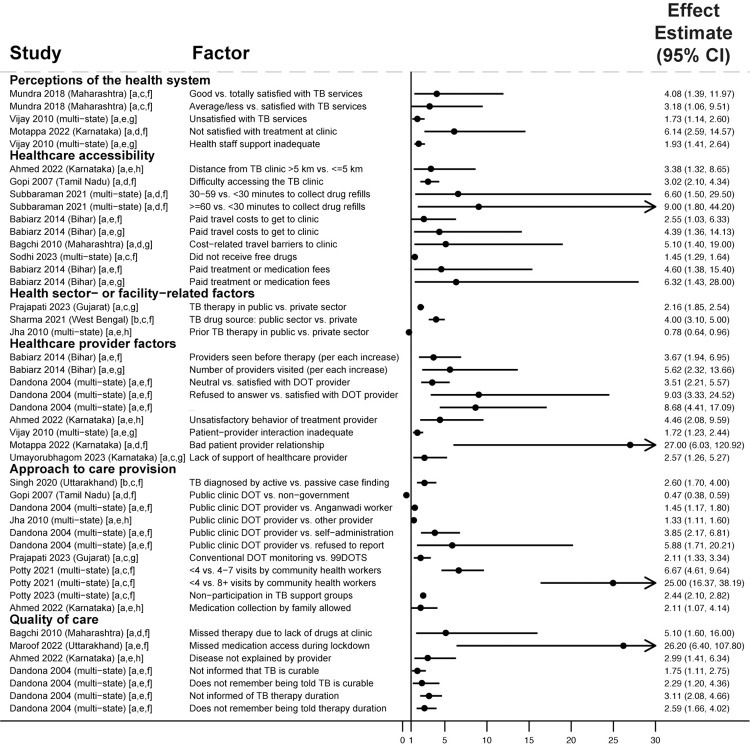
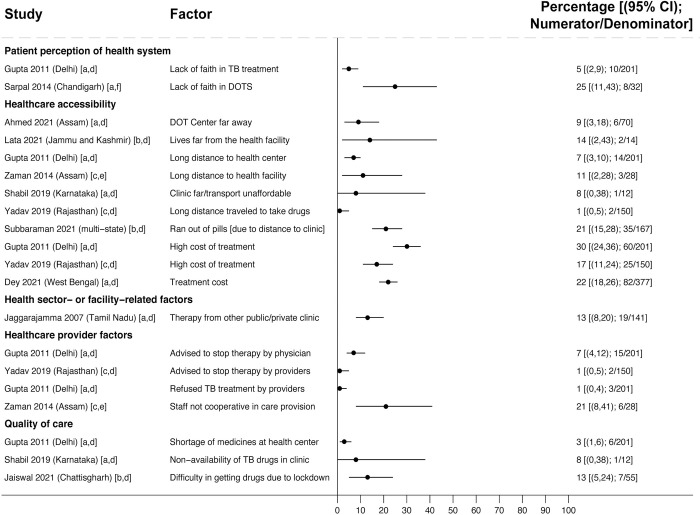
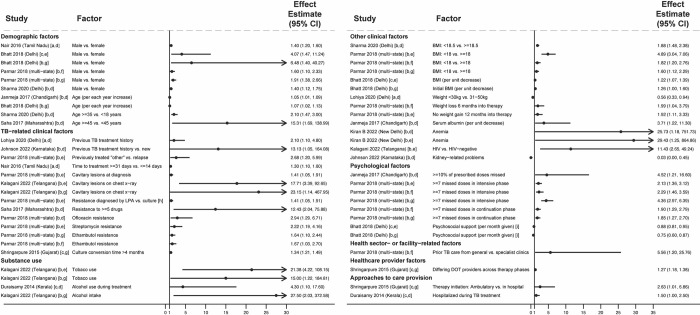
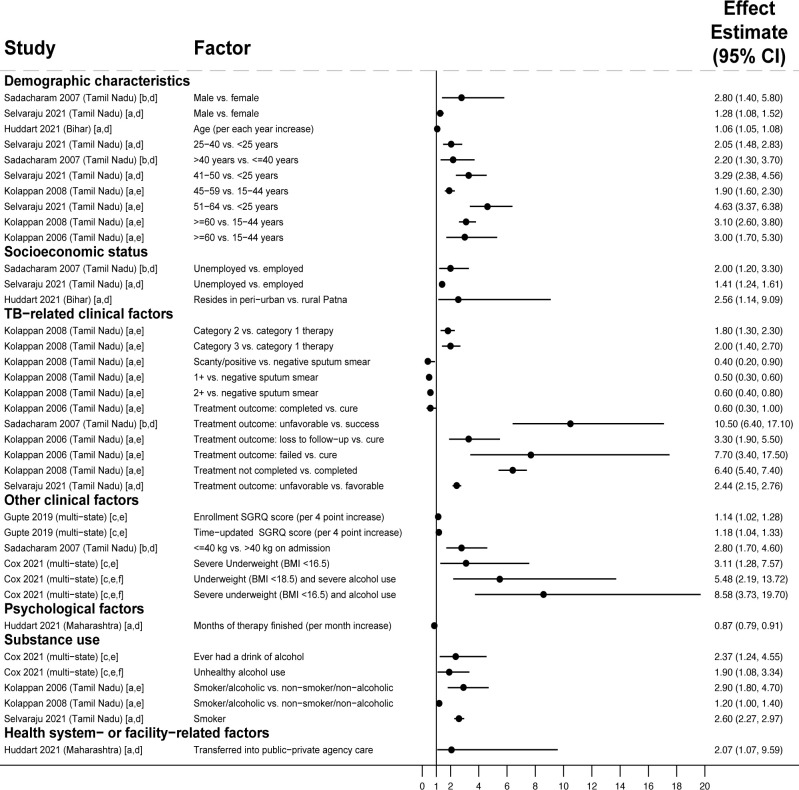
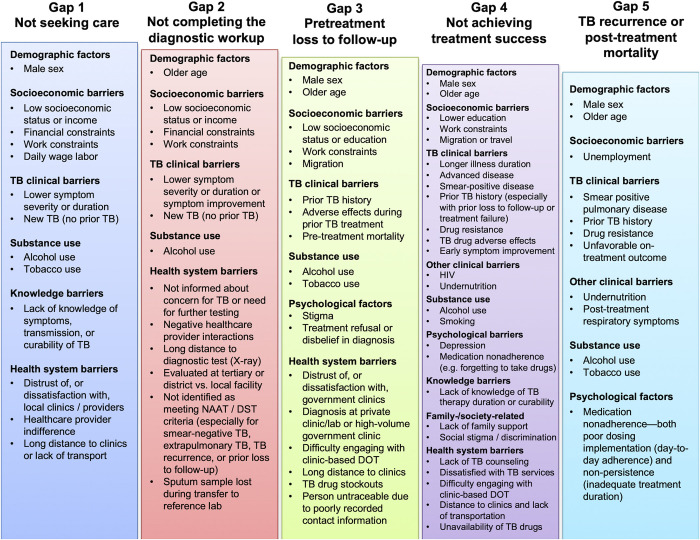
Methods and findings: We defined care cascade gaps as comprising people with confirmed or presumptive TB who did not: start the TB diagnostic workup (Gap 1), complete the workup (Gap 2), start treatment (Gap 3), achieve treatment success (Gap 4), or achieve TB recurrence-free survival (Gap 5). Three systematic searches of PubMed, Embase, and Web of Science from January 1, 2000 to August 14, 2023 were conducted. We identified articles evaluating factors associated with unfavorable outcomes for each gap (reported as adjusted odds, relative risk, or hazard ratios) and, among people experiencing unfavorable outcomes, reasons for these outcomes (reported as proportions), with specific quality or risk of bias criteria for each gap. Findings were organized into person-, family-, and society-, or health system-related factors, using a social-ecological framework. Factors associated with unfavorable outcomes across multiple cascade stages included: male sex, older age, poverty-related factors, lower symptom severity or duration, undernutrition, alcohol use, smoking, and distrust of (or dissatisfaction with) health services. People previously treated for TB were more likely to seek care and engage in the diagnostic workup (Gaps 1 and 2) but more likely to suffer pretreatment loss to follow-up (Gap 3) and unfavorable treatment outcomes (Gap 4), especially those who were lost to follow-up during their prior treatment. For individual care cascade gaps, multiple studies highlighted lack of TB knowledge and structural barriers (e.g., transportation challenges) as contributing to lack of care-seeking for TB symptoms (Gap 1, 14 studies); lack of access to diagnostics (e.g., X-ray), non-identification of eligible people for testing, and failure of providers to communicate concern for TB as contributing to non-completion of the diagnostic workup (Gap 2, 17 studies); stigma, poor recording of patient contact information by providers, and early death from diagnostic delays as contributing to pretreatment loss to follow-up (Gap 3, 15 studies); and lack of TB knowledge, stigma, depression, and medication adverse effects as contributing to unfavorable treatment outcomes (Gap 4, 86 studies). Medication nonadherence contributed to unfavorable treatment outcomes (Gap 4) and TB recurrence (Gap 5, 14 studies). Limitations include lack of meta-analyses due to the heterogeneity of findings and limited generalizability to some Indian regions, given the country's diverse population.
Conclusions: This systematic review illuminates common patterns of risk that shape outcomes for Indians with TB, while highlighting knowledge gaps-particularly regarding TB care for children or in the private sector-to guide future research. Findings may inform targeting of support services to people with TB who have higher risk of poor outcomes and inform multicomponent interventions to close gaps in the care cascade.
Copyright: © 2024 Jhaveri et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
MP is an Academic Editor on PLOS Medicine’s editorial board, and serves as Editor-in-Chief of PLOS Global Public Health. MP also serves as an advisor to the following non-profit agencies in global health: Bill & Melinda Gates Foundation; Foundation for Innovative New Diagnostics; World Health Organization & the Stop TB Partnership. JEH has been a paid consultant for Merck. JEH owns stock in Natera. All other authors have declared that no competing interests exist.
Figures

Similar articles
-
Impact of summer programmes on the outcomes of disadvantaged or 'at risk' young people: A systematic review.Campbell Syst Rev. 2024 Jun 13;20(2):e1406. doi: 10.1002/cl2.1406. eCollection 2024 Jun. Campbell Syst Rev. 2024. PMID: 38873396 Free PMC article. Review.
-
Exploring private sector perspectives on barriers and facilitators in availing tuberculosis care cascade services: a qualitative study from the Indian state.BMC Prim Care. 2024 Jan 2;25(1):5. doi: 10.1186/s12875-023-02244-w. BMC Prim Care. 2024. PMID: 38166734 Free PMC article.
-
The role of counselling in tuberculosis diagnostic evaluation and contact tracing: scoping review and stakeholder consultation of knowledge and research gaps.BMC Public Health. 2022 Jan 28;22(1):190. doi: 10.1186/s12889-022-12556-8. BMC Public Health. 2022. PMID: 35090414 Free PMC article.
-
Improving cascade outcomes for active TB: A global systematic review and meta-analysis of TB interventions.PLoS Med. 2023 Jan 3;20(1):e1004091. doi: 10.1371/journal.pmed.1004091. eCollection 2023 Jan. PLoS Med. 2023. PMID: 36595536 Free PMC article.
-
Prediagnostic loss to follow-up in an active case finding tuberculosis programme: a mixed-methods study from rural Bihar, India.BMJ Open. 2020 May 15;10(5):e033706. doi: 10.1136/bmjopen-2019-033706. BMJ Open. 2020. PMID: 32414819 Free PMC article.
Cited by
-
Contextual factors influencing implementation of tuberculosis digital adherence technologies: a scoping review guided by the RE-AIM framework.BMJ Glob Health. 2025 Feb 13;10(2):e016608. doi: 10.1136/bmjgh-2024-016608. BMJ Glob Health. 2025. PMID: 39947716 Free PMC article.
-
"I consulted so many doctors": the journey of tuberculosis patients in Bengaluru, India, from first symptoms to diagnosis.BMC Health Serv Res. 2025 Mar 18;25(1):397. doi: 10.1186/s12913-025-12547-6. BMC Health Serv Res. 2025. PMID: 40102870 Free PMC article.
-
Global, regional, and national burden of HIV-negative tuberculosis, 1990-2021: findings from the Global Burden of Disease Study 2021.Infect Dis Poverty. 2024 Aug 19;13(1):60. doi: 10.1186/s40249-024-01227-y. Infect Dis Poverty. 2024. PMID: 39155365 Free PMC article.
-
Barriers and facilitators to tuberculosis service access for patients in Bajhang, Nepal: a qualitative study based on focus groups with patients, screening camp visitors, community volunteers and medical doctors.J Health Popul Nutr. 2025 Feb 21;44(1):46. doi: 10.1186/s41043-025-00788-4. J Health Popul Nutr. 2025. PMID: 39985120 Free PMC article.
-
TB treatment delays and associated risk factors in Dushanbe, Tajikistan, 2019-2021.BMC Infect Dis. 2024 Dec 18;24(1):1398. doi: 10.1186/s12879-024-10265-8. BMC Infect Dis. 2024. PMID: 39695401 Free PMC article.
References
-
- World Health Organization. Global tuberculosis report 2023 [Internet]. Geneva, Switzerland: World Health Organization; 2023. Available from: https://www.who.int/teams/global-tuberculosis-programme/tb-reports/globa.... Accessed 2024 Apr 9.
-
- Central TB. Division. India TB report 2020 [Internet]. New Delhi, India: Ministry of Health and Family Welfare; 2020. Available from: https://tbcindia.gov.in/showfile.php?lid=3538. Accessed 2024 Apr 9.
-
- Subbaraman R, Nathavitharana RR, Mayer KH, Satyanarayana S, Chadha VK, Arinaminpathy N, et al.. Constructing care cascades for active tuberculosis: A strategy for program monitoring and identifying gaps in quality of care. PLoS Med. 2019; 16: e1002754. doi: 10.1371/journal.pmed.1002754 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
