

Novel paradigm enables accurate monthly gestational screening to prevent congenital toxoplasmosis and more
- PMID: 38805559
- PMCID: PMC11132520
- DOI: 10.1371/journal.pntd.0011335
Novel paradigm enables accurate monthly gestational screening to prevent congenital toxoplasmosis and more
Abstract
Background: Congenital toxoplasmosis is a treatable, preventable disease, but untreated causes death, prematurity, loss of sight, cognition and motor function, and substantial costs worldwide.
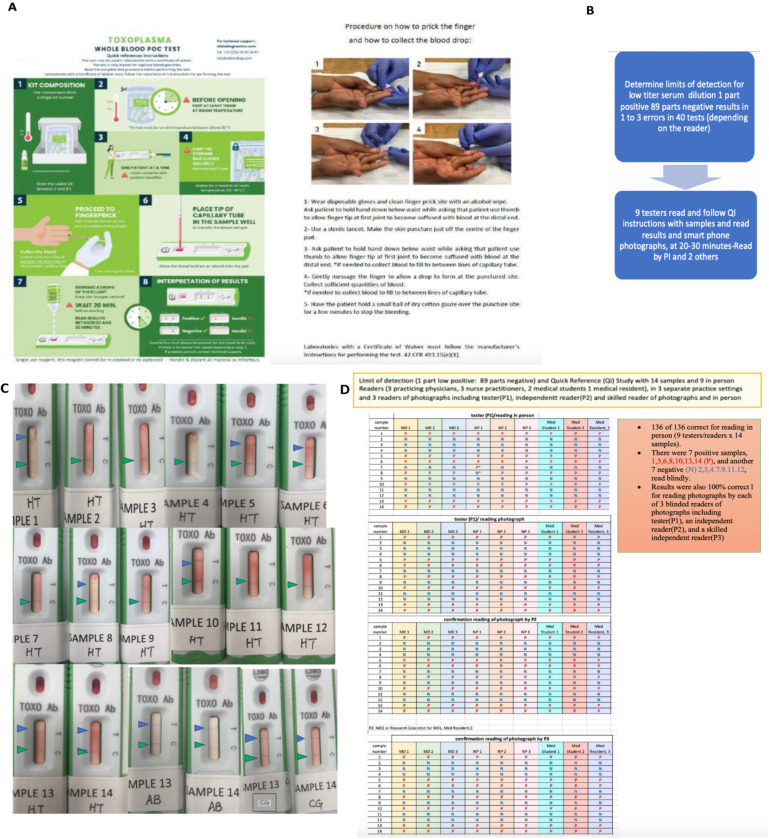
Objectives: We asked whether high performance of an Immunochromatographic-test (ICT) could enable accurate, rapid diagnosis/treatment, establishing new, improved care-paradigms at point-of-care and clinical laboratory.
Methods: Data were obtained in 12 studies/analyses addressing: 1-feasibility/efficacy; 2-false-positives; 3-acceptability; 4-pink/black-line/all studies; 5-time/cost; 6-Quick-Information/Limit-of-detection; 7, 8-acute;-chronic; 9-epidemiology; 10-ADBio; 11,12-Commentary/Cases/Chronology.
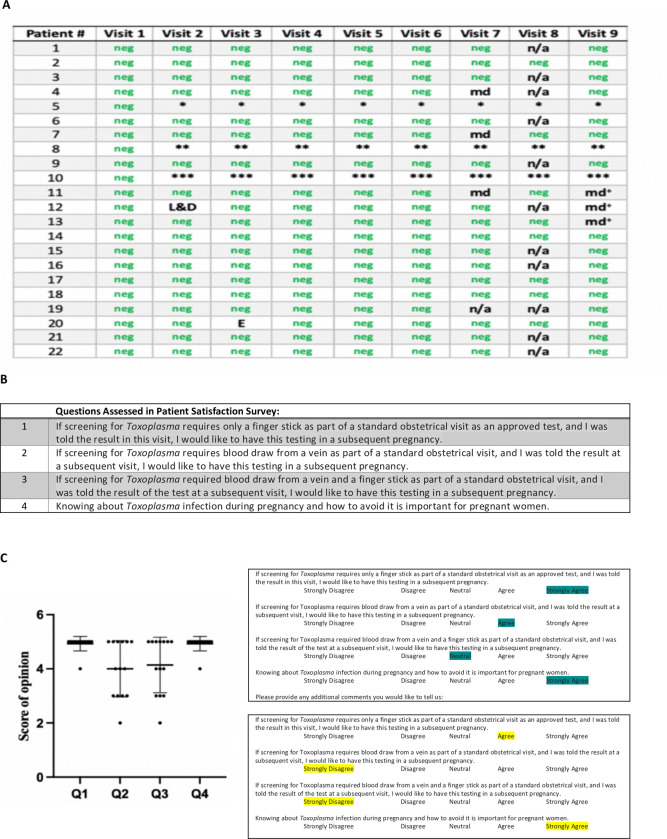
Findings: ICT was compared with gold-standard or predicate-tests. Overall, ICT performance for 1093 blood/4967 sera was 99.2%/97.5% sensitive and 99.0%/99.7% specific. However, in clinical trial, FDA-cleared-predicate tests initially caused practical, costly problems due to false-positive-IgM results. For 58 persons, 3/43 seronegative and 2/15 chronically infected persons had false positive IgM predicate tests. This caused substantial anxiety, concerns, and required costly, delayed confirmation in reference centers. Absence of false positive ICT results contributes to solutions: Lyon and Paris France and USA Reference laboratories frequently receive sera with erroneously positive local laboratory IgM results impeding patient care. Therefore, thirty-two such sera referred to Lyon's Reference laboratory were ICT-tested. We collated these with other earlier/ongoing results: 132 of 137 USA or French persons had false-positive local laboratory IgM results identified correctly as negative by ICT. Five false positive ICT results in Tunisia and Marseille, France, emphasize need to confirm positive ICT results with Sabin-Feldman-Dye-test or western blot. Separate studies demonstrated high performance in detecting acute infections, meeting FDA, CLIA, WHO REASSURED, CEMark criteria and patient and physician satisfaction with monthly-gestational-ICT-screening.
Conclusions/significance: This novel paradigm using ICT identifies likely false positives or raises suspicion that a result is truly positive, rapidly needing prompt follow up and treatment. Thus, ICT enables well-accepted gestational screening programs that facilitate rapid treatment saving lives, sight, cognition and motor function. This reduces anxiety, delays, work, and cost at point-of-care and clinical laboratories.
Trial registration: NCT04474132, https://clinicaltrials.gov/study/NCT04474132 ClinicalTrials.gov.
Copyright: © 2024 Zhou et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
We have read the journal’s policy and the authors of this manuscript have the following competing interests: DL and RP are/were affiliated with LDBIO Diagnostics, DL is the scientist and CEO share holder and RP was the R&D Director Scientist until January 13, 2023. A patent application was submitted by DL with the scientists at the University of Chicago and in Lyon, France in August 2018. This application is pending review in the United States in accordance with US Bayh Dole Laws. This is for the development of the whole blood point of care test and the practical clinical utility of the ICT to guide treatment for gestational infection to prevent congenital toxoplasmosis. This is to insure its continued high-quality performance and reproducibility of the results described herein. It is pending in review at the US patent office. All other authors have declared no conflict of interest.
Figures






Update of
-
Novel paradigm enables accurate monthly gestational screening to prevent congenital toxoplasmosis and more.medRxiv [Preprint]. 2023 May 10:2023.04.26.23289132. doi: 10.1101/2023.04.26.23289132. medRxiv. 2023. Update in: PLoS Negl Trop Dis. 2024 May 28;18(5):e0011335. doi: 10.1371/journal.pntd.0011335. PMID: 37162985 Free PMC article. Updated. Preprint.
References
-
- McLeod R, Lykins J, Noble AG, Rabiah P, Swisher C, Heydemann P, et al. Management of Congenital Toxoplasmosis. Curr Pediatr Rep 2014; 2:166–194
-
- Mandelbrot L, Kieffer F, Sitta R, Laurichesse-Delmas H, Winer N, Mesnard L, et al.. Prenatal therapy with pyrimethamine + sulfadiazine vs spiramycin to reduce placental transmission of toxoplasmosis: a multicenter, randomized trial. Am J Obstet Gynecol 2018; 219(4): 386.e1-386.e9. doi: 10.1016/j.ajog.2018.05.031 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
