

First and second-generation endometrial ablation devices: A network meta-analysis
- PMID: 38806429
- PMCID: PMC11138282
- DOI: 10.1136/bmjopen-2022-065966
First and second-generation endometrial ablation devices: A network meta-analysis
Abstract
Objective: First-generation and second-generation endometrial ablation (EA) techniques, along with medical treatment and invasive surgery, are considered successful lines of management for abnormal uterine bleeding (AUB). We set out to determine the efficacy of first and second-generation ablation techniques compared with medical treatment, invasive surgery and different modalities of the EA techniques themselves.
Design: Systematic review and network meta-analysis using a frequentist network.
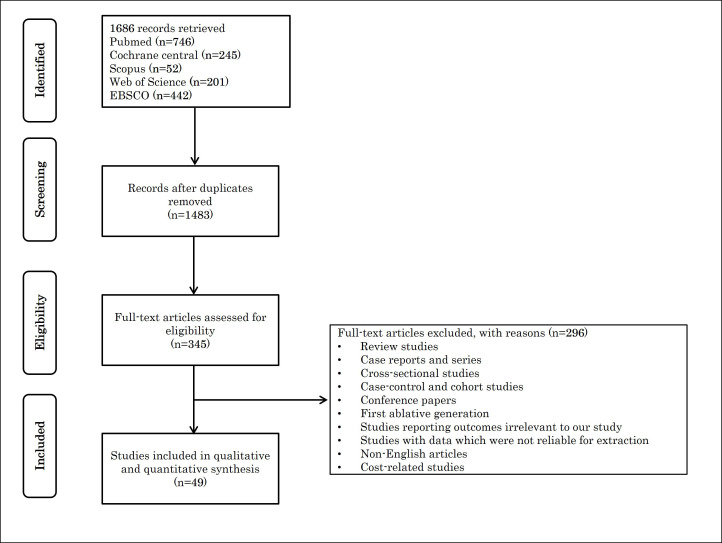
Data sources: We searched Medline (Ovid), PubMed, ClinicalTrials.gov, Cochrane CENTRAL, Web of Science, EBSCO and Scopus for all published studies up to 1 March 2021 using relevant keywords.
Eligibility criteria: We included all randomised controlled trials (RCTs) that compared premenopausal women with AUB receiving the intervention of second-generation EA techniques.
Data extraction and synthesis: 49 high-quality RCTs with 8038 women were included. We extracted and pooled the data and then analysed to estimate the network meta-analysis models within a frequentist framework. We used the random-effects model of the netmeta package in R (V.3.6.1) and the 'Meta-Insight' website.
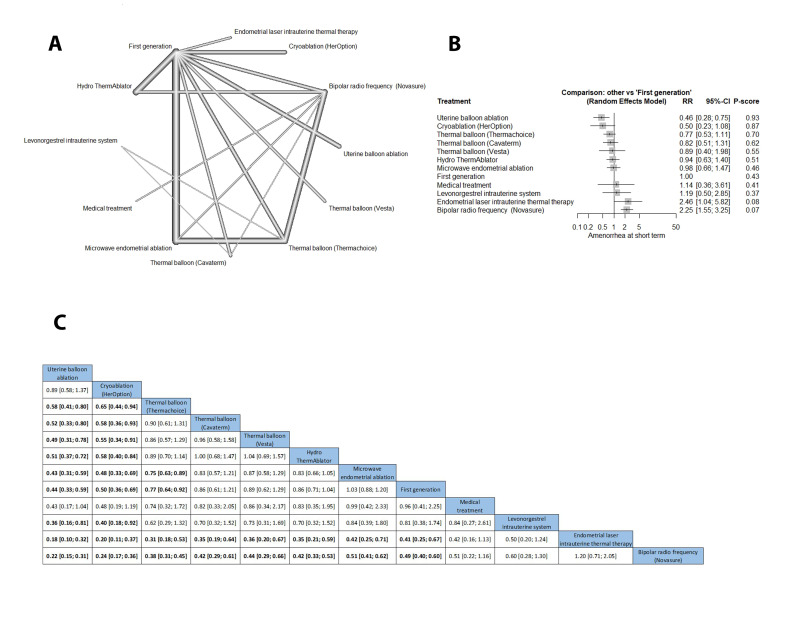
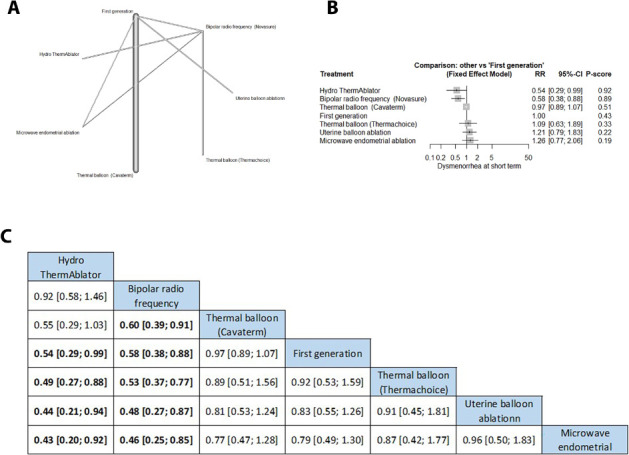
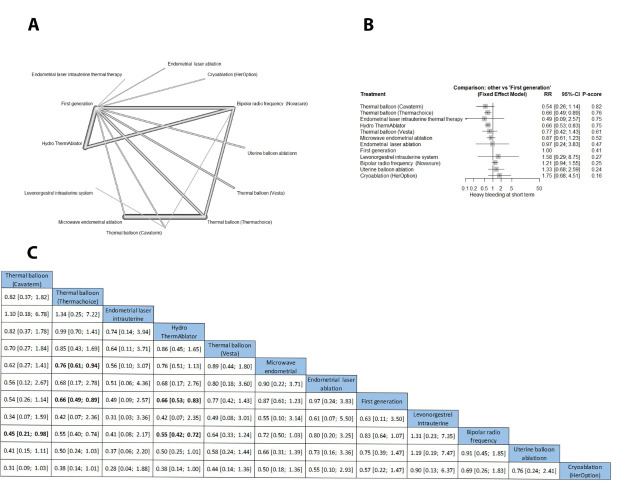
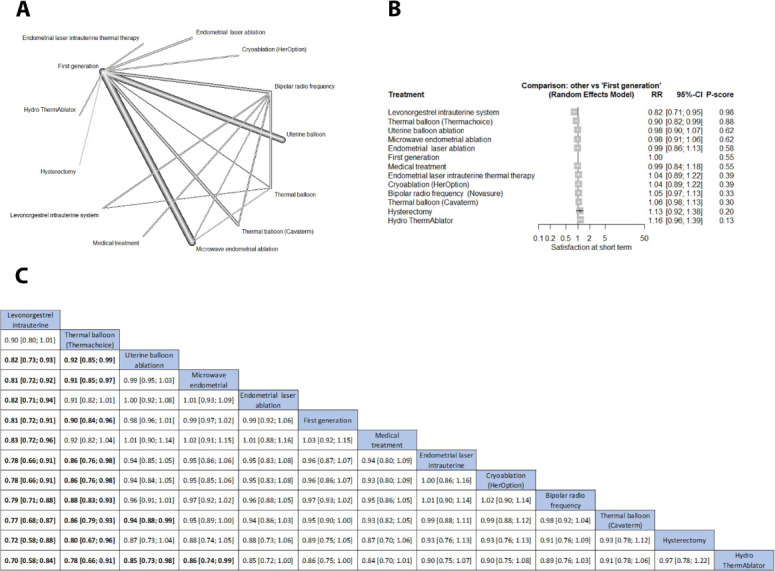
Results: Our network meta-analysis showed many varying results according to specific outcomes. The uterine balloon ablation had significantly higher amenorrhoea rates than other techniques in both short (hydrothermal ablation (risk ratio (RR)=0.51, 95% CI 0.37; 0.72), microwave ablation (RR=0.43, 95% CI 0.31; 0.59), first-generation techniques (RR=0.44, 95% CI 0.33; 0.59), endometrial laser intrauterine therapy (RR=0.18, 95% CI 0.10; 0.32) and bipolar radio frequency treatments (RR=0.22, 95% CI 0.15; 0.31)) and long-term follow-up (microwave ablation (RR=0.11, 95% CI 0.01; 0.86), bipolar radio frequency ablation (RR=0.12, 95% CI 0.02; 0.90), first generation (RR=0.12, 95% CI 0.02; 0.90) and endometrial laser intrauterine thermal therapy (RR=0.04, 95% CI 0.01; 0.36)). When calculating efficacy based only on calculated bleeding scores, the highest scores were achieved by cryoablation systems (p-score=0.98).
Conclusion: Most second-generation EA systems were superior to first-generation systems, and statistical superiority between devices depended on which characteristic was measured (secondary amenorrhoea rate, treatment of AUB, patient satisfaction or treatment of dysmenorrhoea). Although our study was limited by a paucity of data comparing large numbers of devices, we conclude that there is no evidence at this time that any one of the examined second-generation systems is clearly superior to all others.
Keywords: Community gynaecology; GYNAECOLOGY; Minimally invasive surgery.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures

Similar articles
-
Drugs for preventing postoperative nausea and vomiting in adults after general anaesthesia: a network meta-analysis.Cochrane Database Syst Rev. 2020 Oct 19;10(10):CD012859. doi: 10.1002/14651858.CD012859.pub2. Cochrane Database Syst Rev. 2020. PMID: 33075160 Free PMC article.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
-
Ablative and non-surgical therapies for early and very early hepatocellular carcinoma: a systematic review and network meta-analysis.Health Technol Assess. 2023 Dec;27(29):1-172. doi: 10.3310/GK5221. Health Technol Assess. 2023. PMID: 38149643 Free PMC article.
-
Three-dimensional saline infusion sonography compared to two-dimensional saline infusion sonography for the diagnosis of focal intracavitary lesions.Cochrane Database Syst Rev. 2017 May 5;5(5):CD011126. doi: 10.1002/14651858.CD011126.pub2. Cochrane Database Syst Rev. 2017. PMID: 28472862 Free PMC article.
-
Progesterone or progestogen-releasing intrauterine systems for heavy menstrual bleeding.Cochrane Database Syst Rev. 2005 Oct 19;(4):CD002126. doi: 10.1002/14651858.CD002126.pub2. Cochrane Database Syst Rev. 2005. Update in: Cochrane Database Syst Rev. 2015 Apr 30;(4):CD002126. doi: 10.1002/14651858.CD002126.pub3. PMID: 16235297 Updated.
References
-
- Illingworth P. Chapter 129 - Amenorrhea, Anovulation, and dysfunctional uterine bleeding. Jameson JL, De Groot L-E, eds. 6th edn. Philadelphia: W.B. Saunders, 2010: 2341–55.
-
- Pakpreo P. Dysfunctional uterine bleeding. Garfunkel LC, Kaczorowski JM, Christy C-P, eds. 2nd edn. Philadelphia: Mosby, 2007: 177–8.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources