

The road to tailored adjuvant chemotherapy for all four non-pancreatic periampullary cancers: An international multimethod cohort study
- PMID: 38806725
- PMCID: PMC11231293
- DOI: 10.1038/s41416-024-02692-w
The road to tailored adjuvant chemotherapy for all four non-pancreatic periampullary cancers: An international multimethod cohort study
Abstract
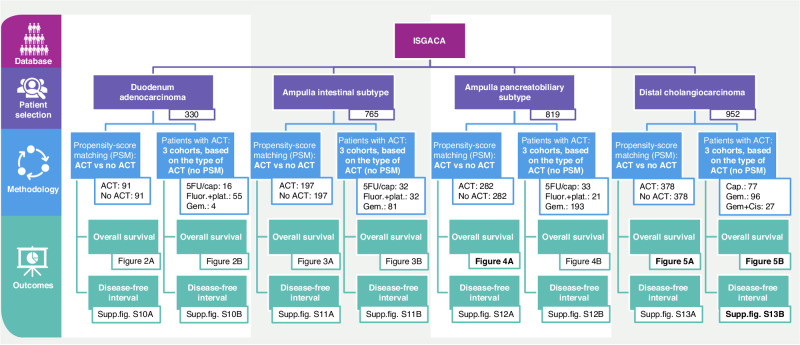
Background: Despite differences in tumour behaviour and characteristics between duodenal adenocarcinoma (DAC), the intestinal (AmpIT) and pancreatobiliary (AmpPB) subtype of ampullary adenocarcinoma and distal cholangiocarcinoma (dCCA), the effect of adjuvant chemotherapy (ACT) on these cancers, as well as the optimal ACT regimen, has not been comprehensively assessed. This study aims to assess the influence of tailored ACT on DAC, dCCA, AmpIT, and AmpPB.
Patients and methods: Patients after pancreatoduodenectomy for non-pancreatic periampullary adenocarcinoma were identified and collected from 36 tertiary centres between 2010 - 2021. Per non-pancreatic periampullary tumour type, the effect of adjuvant chemotherapy and the main relevant regimens of adjuvant chemotherapy were compared. The primary outcome was overall survival (OS).
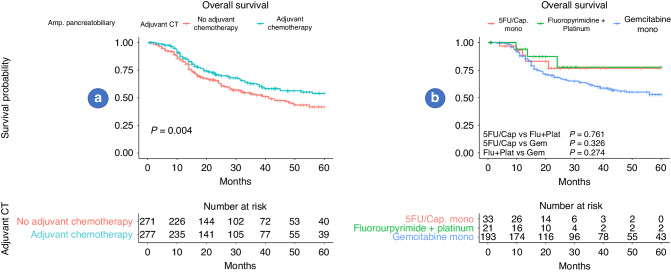
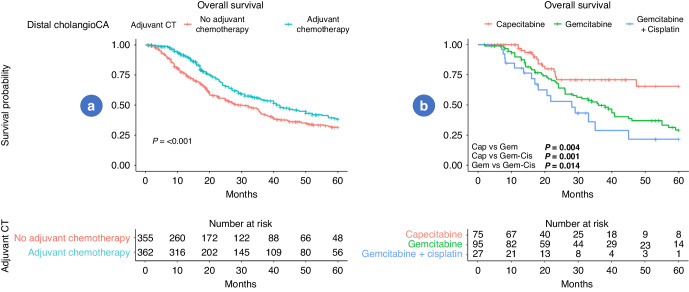
Results: The study included a total of 2866 patients with DAC (n = 330), AmpIT (n = 765), AmpPB (n = 819), and dCCA (n = 952). Among them, 1329 received ACT, and 1537 did not. ACT was associated with significant improvement in OS for AmpPB (P = 0.004) and dCCA (P < 0.001). Moreover, for patients with dCCA, capecitabine mono ACT provided the greatest OS benefit compared to gemcitabine (P = 0.004) and gemcitabine - cisplatin (P = 0.001). For patients with AmpPB, no superior ACT regime was found (P > 0.226). ACT was not associated with improved OS for DAC and AmpIT (P = 0.113 and P = 0.445, respectively).
Discussion: Patients with resected AmpPB and dCCA appear to benefit from ACT. While the optimal ACT for AmpPB remains undetermined, it appears that dCCA shows the most favourable response to capecitabine monotherapy. Tailored adjuvant treatments are essential for enhancing prognosis across all four non-pancreatic periampullary adenocarcinomas.
© 2024. The Author(s), under exclusive licence to Springer Nature Limited.
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Adsay V, Ohike N, Tajiri T, Kim GE, Krasinskas A, Balci S, et al. Ampullary region carcinomas: definition and site specific classification with delineation of four clinicopathologically and prognostically distinct subsets in an analysis of 249 cases. Am J Surg Pathol. 2012;36:1592–608. - PubMed
-
- Lerch MM, Domschke W. Abraham Vater of the ampulla (papilla) of Vater. Gastroenterology. 2000;118:379. - PubMed
-
- Sarmiento JM, Nagomey DM, Sarr MG, Farnell MB. Periampullary cancers: are there differences? Surg Clin North Am. 2001;81:543–55. - PubMed
-
- Schnelldorfer T, Ware AL, Sarr MG, Smyrk TC, Zhang L, Qin R, et al. Long-term survival after pancreatoduodenectomy for pancreatic adenocarcinoma: is cure possible? Ann Surg. 2008;247:456–62. - PubMed
-
- Han SS, Jang JY, Kim SW, Kim WH, Lee KU, Park YH. Analysis of long-term survivors after surgical resection for pancreatic cancer. Pancreas. 2006;32:271–5. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
