

In Vivo Comparison of the Efficacy and Duration of Local Antibiotics on Smooth, Textured and Polyurethane Implant Surfaces
- PMID: 38806833
- PMCID: PMC11739227
- DOI: 10.1007/s00266-024-04090-2
In Vivo Comparison of the Efficacy and Duration of Local Antibiotics on Smooth, Textured and Polyurethane Implant Surfaces
Abstract
Background: Capsular contracture is one of the most common complications after breast surgery involving silicone implants. The most likely cause of this condition is biofilm formation. In this study, the efficacy of local antibiotherapy against biofilm formation on implant surfaces was investigated.
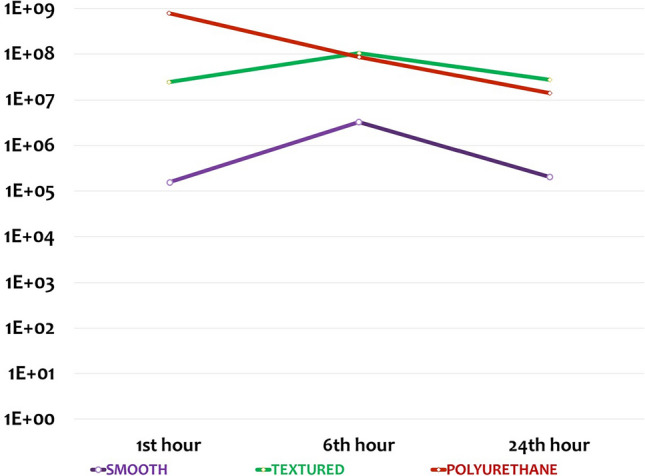
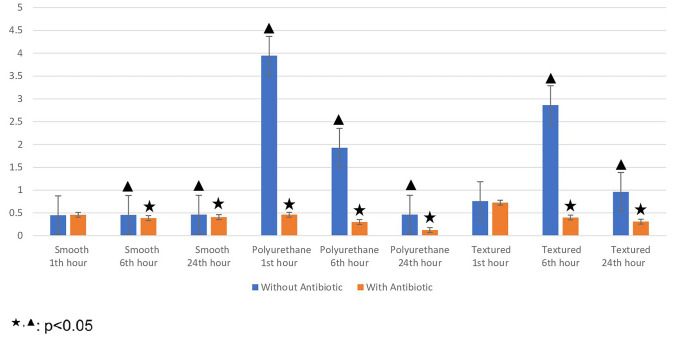
Methods: Thirty-six rats were divided into six groups. Three pockets were created on the dorsum of each rat, and 1 × 2 cm implant surface samples from smooth, polyurethane and textured implants were randomly placed into pockets. All samples were inoculated with staphylococcus epidermidis. In groups 1-2-3, inoculated samples were placed into the pockets and removed after 1, 6 and 24 h, respectively. In groups 4-5-6, inoculated samples immersed with rifamycin were placed and removed after 1, 6 and 24 h, respectively. Bacterial load was measured with plate count method.
Results: Bacterial load was lower in groups 4-5-6 than in groups 1-2-3 (p < 0.05). In groups 4-5-6, bacterial load was lower for polyurethane than for textured surfaces at all time points (1, 6 and 24 h; p < 0.05). Again, in groups 4-5-6, bacterial load was lower for smooth than for textured surfaces at 24 h (p < 0.05). In groups 4-5-6, bacterial load was lower for polyurethane than for smooth surfaces at all time points, but difference was not statistically significant (1, 6 and 24 h; p < 0.05).
Conclusion: The results suggest that local antibiotic therapy was effective in reducing the bacterial load on all surfaces. The effectiveness of local rifamycin on the polyurethane surface was higher, and the duration of activity was longer than other surfaces.
No level assigned: This journal requires that authors assign a level of evidence to each article. For a full description of these evidence-based medicine ratings, please refer to the Table of contents or the online Instructions to Authors www.springer.com/00266 .
Keywords: Antibiotics; BIA-ALCL; Bacteria; Biofilm; Breast implants; Microorganism; Polyurethane textured smooth.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: The authors declare no potential conflicts of interest with respect to the research, authorship and publication of this article. Ethical Approval: Ethical approval was obtained from the Gazi University Local Ethical Committee of Animal Experiments (Approval ID: G.U.ET-20.027). Informed Consent: For this type of study, informed consent is not required.
Figures




References
-
- Chong SJ, Deva AK (2015) Understanding the etiology and prevention of capsular contracture: translating science into practice. Clin Plast Surg 42(4):427–436. 10.1016/j.cps.2015.06.007 - PubMed
-
- Gampper TJ, Khoury H, Gottlieb W, Morgan RF (2007) Silicone gel implants in breast augmentation and reconstruction. Ann Plast Surg 59(5):581–590. 10.1097/01.sap.0000258970.31562.5d - PubMed
-
- Adams WP Jr (2009) Capsular contracture: What is it? What causes it? How can it be prevented and managed? Clin Plast Surg 36(1):119–126. 10.1016/j.cps.2008.08.007 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
