

Synchronous liver metastasis at initial diagnosis of adrenal pheochromocytoma by CT: A case report
- PMID: 38807675
- PMCID: PMC11130753
- DOI: 10.3892/ol.2024.14462
Synchronous liver metastasis at initial diagnosis of adrenal pheochromocytoma by CT: A case report
Abstract
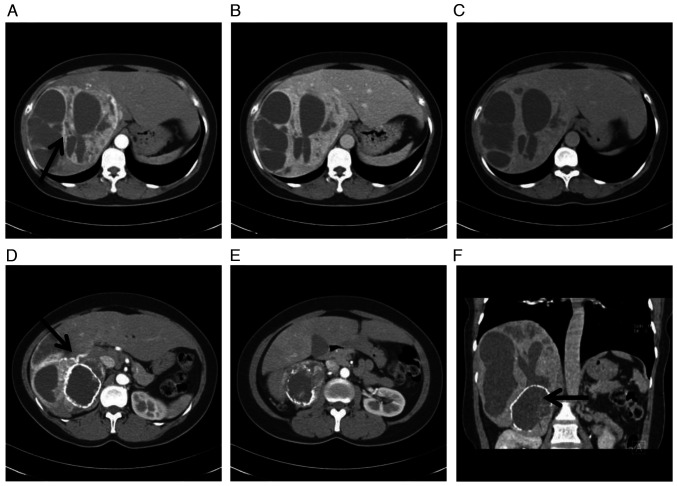
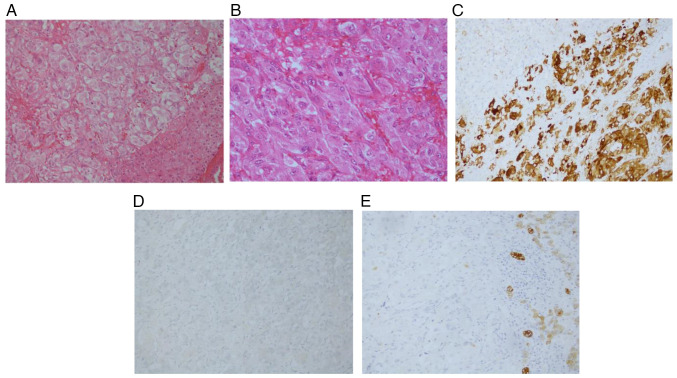
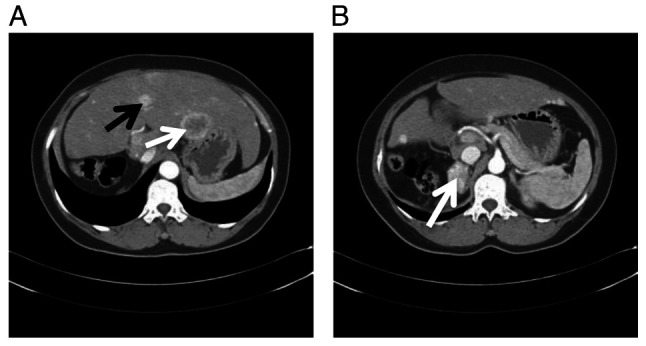
Pheochromocytoma is a tumor of the sympathetic nervous system, characterized by atypical symptoms and signs. Pheochromocytoma metastases can be found in various tissues and organs. However, synchronous metastasis at the initial diagnosis of pheochromocytoma is rare. The present study described a case with synchronous liver metastasis at the initial diagnosis of adrenal pheochromocytoma based on imaging findings. A 41-year-old woman presented with liver pain and fatigue for 1 month. Physical examination showed increased blood pressure and heart rate with sinus tachycardia. Laboratory examination revealed normal levels of liver tumor markers and increased levels of serum or urine epinephrine and norepinephrine. CT examination revealed a large cystic solid mass in the right lobe of the liver and right adrenal gland, and the solid part of the mass was enhanced after enhancement. The pathological diagnosis was pheochromocytoma of the right adrenal gland with liver metastasis. The patient underwent right hepatectomy and right adrenal tumor resection. During the postoperative follow-up, the patient's blood pressure and catecholamine levels were within the normal range. Three years after surgery, the CT examination revealed multiple liver metastases. Chemotherapy was administered to the patient. A year later, re-examination revealed an increase and enlargement of the metastases, and the mass of the right adrenal gland remained similar to the previous one. After 6 months of follow-up, the patient succumbed to recurrence and metastasis. Preoperative diagnosis of metastatic pheochromocytoma is challenging. This case mainly emphasizes that imaging findings can help the clinical diagnosis of metastatic pheochromocytoma.
Keywords: adrenal gland metastasis; liver metastasis; metastatic pheochromocytoma.
Copyright © 2024, Spandidos Publications.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources