

Lymph node myeloid sarcoma with TP53‑associated myelodysplastic syndrome: A case report
- PMID: 38807682
- PMCID: PMC11130743
- DOI: 10.3892/ol.2024.14458
Lymph node myeloid sarcoma with TP53‑associated myelodysplastic syndrome: A case report
Abstract
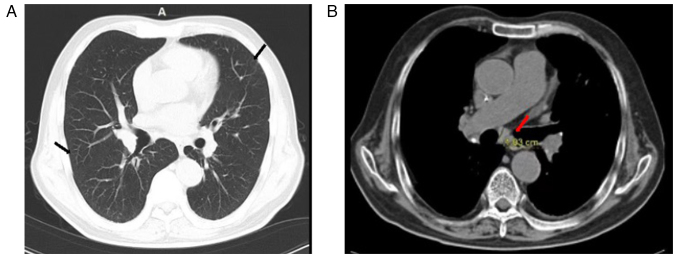
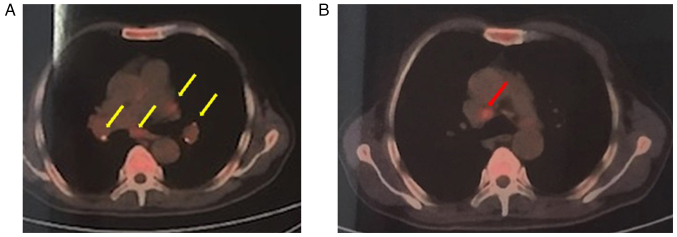
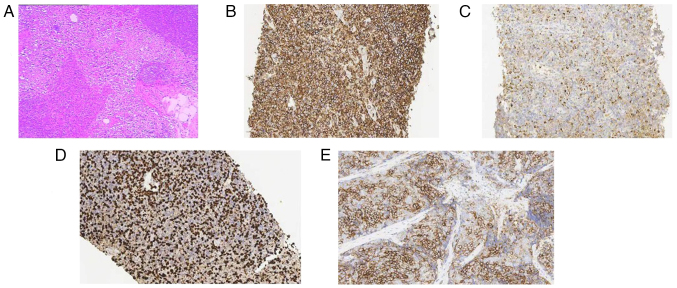
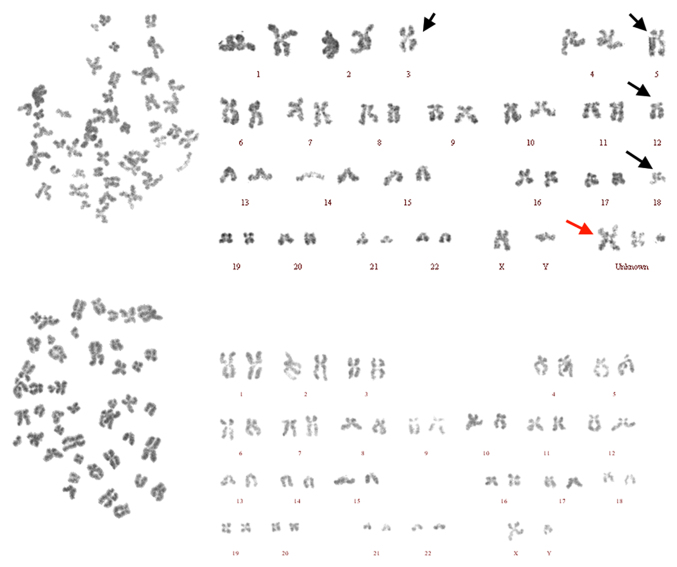
Myeloid sarcoma (MS) is a rare extramedullary tumor mass that carries a high risk of progression to acute myeloid leukemia (AML), and patients with MS are commonly treated with the AML regimen. However, MS is frequently misdiagnosed due to its lack of clinical specificity. Patients with MS who harbor tumor protein p53 (TP53) mutations and complex karyotypes are considered to have a poorer prognosis. The present study reports a case of lymph node MS with TP53 (V173G)-related myelodysplastic syndrome (MDS). The mass was first considered to be a lymphoma and treated as such. However, following immunohistochemical analysis, which revealed cells positive for CD43, myeloperoxidase and CD117, the patient was later diagnosed with MS combined with MDS. The patient went into complete remission after the first cycle of chemotherapy, and showed a decrease in platelet, red blood cell and white blood cell counts following the second cycle of chemotherapy. After the third chemotherapy, agranulocytosis occurred, leading to refractory pneumonia and eventually death due to respiratory failure. MS with TP53-related MDS has a low incidence rate, a poor prognosis and a short survival time. The clinical manifestations of MS are non-specific and easy to misdiagnose, leading to delayed diagnosis and treatment, and ultimately worsening the prognosis of the patients. Therefore, a lymph node biopsy should be performed as soon as possible for patients with lymph node enlargement, and early treatment should be carried out to prolong the survival period.
Keywords: TP53; fever; lymph node; myelodysplastic syndrome; myeloid sarcoma.
Copyright: © 2024 Mao and Deng.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
Acute myeloid leukemia or myelodysplastic syndrome with chromosome 17 abnormalities and long-term outcomes with or without hematopoietic stem cell transplantation.Leuk Res. 2020 Aug;95:106402. doi: 10.1016/j.leukres.2020.106402. Epub 2020 Jun 18. Leuk Res. 2020. PMID: 32590108
-
Double minute chromosomes in acute myeloid leukemia and myelodysplastic syndromes are associated with complex karyotype, monosomal karyotype, TP53 deletion, and TP53 mutations.Leuk Lymphoma. 2021 Oct;62(10):2466-2474. doi: 10.1080/10428194.2021.1919663. Epub 2021 Apr 27. Leuk Lymphoma. 2021. PMID: 33904352
-
Bladder Myeloid Sarcoma with TP53 mutated Myelodysplastic Syndrome/Myeloproliferative Neoplasm Overlap syndrome: Response to Decitabine-Venetoclax regimen.Leuk Res Rep. 2021 Dec 14;17:100286. doi: 10.1016/j.lrr.2021.100286. eCollection 2022. Leuk Res Rep. 2021. PMID: 34976720 Free PMC article.
-
Myeloid sarcoma: an uncommon presentation of myeloid neoplasms; a case series of 4 rare cases reported in a tertiary care institute.Autops Case Rep. 2021 Nov 5;11:e2021339. doi: 10.4322/acr.2021.339. eCollection 2021. Autops Case Rep. 2021. PMID: 34805008 Free PMC article. Review.
-
Extramedullary myeloid cell tumors in myelodysplastic-syndromes: not a true indication of impending acute myeloid leukemia.Leuk Lymphoma. 1996 Mar;21(1-2):153-9. doi: 10.3109/10428199609067593. Leuk Lymphoma. 1996. PMID: 8907283 Review.
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous