

Trends in Immediate Lymphatic Reconstruction
- PMID: 38807806
- PMCID: PMC11131141
- DOI: 10.7759/cureus.59194
Trends in Immediate Lymphatic Reconstruction
Abstract
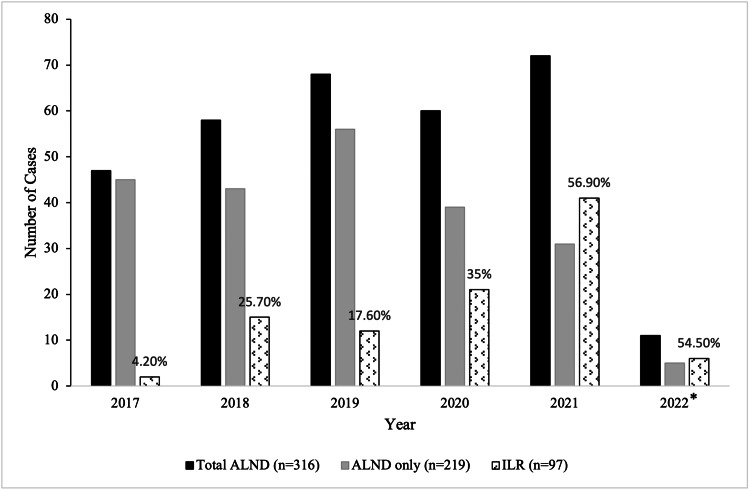
Background and objective Immediate lymphatic reconstruction (ILR) is emerging as a useful adjunct after axillary lymph node dissection (ALND), leading to a decrease in lymphedema rates from 30 to 3-13% in breast cancer patients. ILR requires coordination between two surgical specialties for oncologic ALND and microsurgical axillary lymphatic anastomosis. This study aimed to assess the trends in the frequency of ILR performed after ALND at our institution. Methods This study involved a retrospective review of breast cancer patients undergoing ALND with and without ILR at our institution (2017-2022). Data on patient demographics, tumor characteristics, and treatments received were gathered and analyzed. Results A total of 316 patients underwent ALND at our institution and 30.7% (97/316) of them received ILR. There was no significant difference in clinical breast cancer stages between patients who underwent ALND with or without ILR (p>0.05). Neoadjuvant chemotherapy was given to 51.1% (112/219) of patients with ALND only compared to 60.8% (59/97) of patients who underwent ALND with ILR (p=0.09). All patients received adjuvant radiation therapy. ILR was performed after ALND in 4.2% (2/47) in 2017, 25.8% (3/58) in 2018, 17.6% (12/68) in 2019, 35% (21/60) in 2020, 56.9% (41/72) in 2021, and 54.5% (6/11) in 2022. When comparing the first year of the ILR program with the last year of the study period, the odds ratio of receiving ILR after ALND was 1.8 (p=0.04). Conclusions The frequency of performing ILR after ALND in breast cancer patients at our institution witnessed a substantial increase during the study period. The implementation of an established ILR program at an institution can increase procedure uptake accompanied by continued growth in utilization.
Keywords: alnd: - axillary lymph node dissection; axillary lymphadenectomy; breast cancer related lymphedema; breast lymphedema; lympho-venous-anastomosis.
Copyright © 2024, Ahmed et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- Lymphedema incidence after axillary lymph node dissection: quantifying the impact of radiation and the lymphatic microsurgical preventive healing approach. Johnson AR, Kimball S, Epstein S, et al. Ann Plast Surg. 2019;82:0–41. - PubMed
-
- Single institution experience with lymphatic microsurgical preventive healing approach (LYMPHA) for the primary prevention of lymphedema. Feldman S, Bansil H, Ascherman J, et al. Ann Surg Oncol. 2015;22:3296–3301. - PubMed
-
- Immediate lymphatic reconstruction. Johnson AR, Singhal D. J Surg Oncol. 2018;118:750–757. - PubMed
-
- Lymphatic microsurgical preventing healing approach (LYMPHA) for primary surgical prevention of breast cancer-related lymphedema: over 4 years follow-up. Boccardo F, Casabona F, De Cian F, et al. Microsurgery. 2014;34:421–424. - PubMed
LinkOut - more resources
Full Text Sources