

Membranous urethral length is the single independent predictor of urinary continence recovery at 12 months following Retzius-sparing robot-assisted radical prostatectomy
- PMID: 38809307
- PMCID: PMC11136784
- DOI: 10.1007/s11701-024-01986-8
Membranous urethral length is the single independent predictor of urinary continence recovery at 12 months following Retzius-sparing robot-assisted radical prostatectomy
Abstract
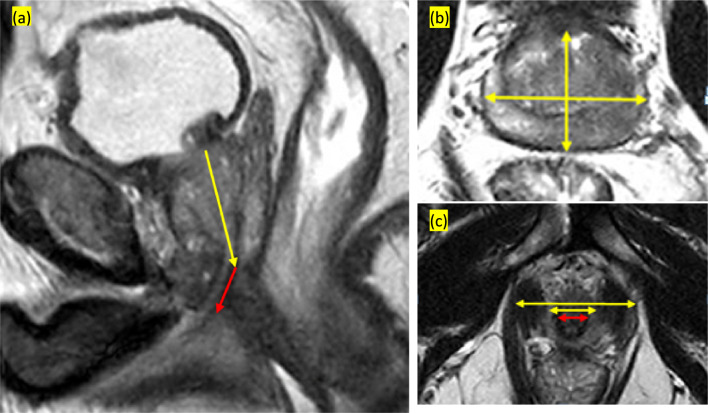
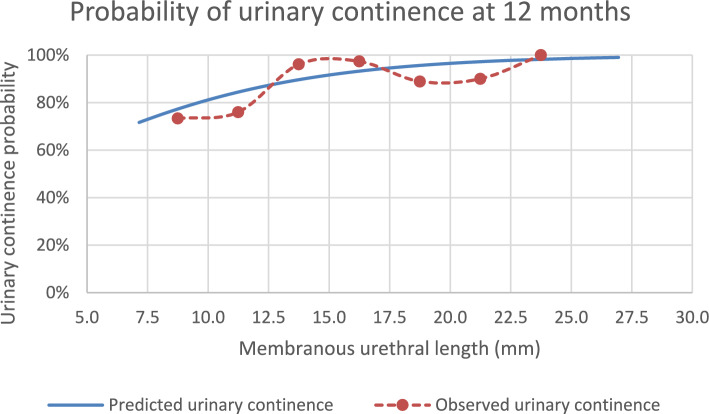
The influence of anatomical parameters on urinary continence (UC) after Retzius-sparing robot-assisted radical prostatectomy (RS-RARP) remains uncharted. Our objective was to evaluate their association with UC at 3, 6 and 12 months post-operatively. Data from patients who underwent RS-RARP were prospectively collected. Continence was defined as no pad use. Anatomic variables were measured on preoperative magnetic resonance imaging (MRI). Regression analyses were performed to identify predictors of UC at each time point. We included 158 patients with a median age of 60 years, most of whom had a localized tumor (≤ cT2). On multivariate analyses, at 3 months post-surgery, urinary incontinence (UI) rises with age, odds ratio (OR) 1.07 [95% confidence interval (CI) 1.004-1.142] and with prostate volume (PV), OR 1.029 (95% CI 1.006-1.052); it reduces with longer membranous urethral length (MUL), OR 0.875 (95% CI 0.780-0.983) and with higher membranous urethral volume (MUV), OR 0.299 (95% CI 0.121-0.737). At 6 months, UI rises with PV, OR 1.033 (95% CI 1.011-1.056) and decreases with MUV, OR 0.1504 (95% CI 0.050-0.444). Significantly, at 12 months post-surgery, the only predictor of UI is MUL, OR 0.830 (95% CI 0.706-0.975), establishing a threshold associated with a risk of UI of 5% (MUL > 15 mm) in opposition to a risk of 25% (MUL < 10 mm). This single institutional study requires external validation. To our knowledge, this is the first prospective cohort study supporting MUL as the single independent predictor of UC at 12 months post-surgery. By establishing MUL thresholds, we enable precise patient counseling.
Keywords: Magnetic resonance imaging; Prognostic tool; Prostate cancer; Retzius-sparing robot-assisted radical prostatectomy; Urinary incontinence.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
The author declares that have no conflict of interest.
Figures
Similar articles
-
Association of bi-parametric MRI measures with continence after robot-assisted radical prostatectomy.BJU Int. 2025 Apr;135(4):603-610. doi: 10.1111/bju.16594. Epub 2024 Nov 29. BJU Int. 2025. PMID: 39611435 Free PMC article.
-
Association Between Preoperative Magnetic Resonance Imaging-based Urethral Parameters and Continence Recovery Following Robot-assisted Radical Prostatectomy.Eur Urol Focus. 2020 Sep 15;6(5):1013-1020. doi: 10.1016/j.euf.2019.01.011. Epub 2019 Jan 25. Eur Urol Focus. 2020. PMID: 30691961
-
A Pragmatic Randomized Controlled Trial Examining the Impact of the Retzius-sparing Approach on Early Urinary Continence Recovery After Robot-assisted Radical Prostatectomy.Eur Urol. 2017 Nov;72(5):677-685. doi: 10.1016/j.eururo.2017.04.029. Epub 2017 May 6. Eur Urol. 2017. PMID: 28483330 Clinical Trial.
-
Membranous urethral length and urinary incontinence following robot-assisted radical prostatectomy: a systematic review and meta-analysis.BJU Int. 2024 Jun;133(6):646-655. doi: 10.1111/bju.16170. Epub 2023 Sep 16. BJU Int. 2024. PMID: 37667431
-
Retzius-sparing versus standard robotic-assisted laparoscopic prostatectomy for the treatment of clinically localized prostate cancer.Cochrane Database Syst Rev. 2020 Aug 18;8(8):CD013641. doi: 10.1002/14651858.CD013641.pub2. Cochrane Database Syst Rev. 2020. PMID: 32813279 Free PMC article.
Cited by
-
Development and validation of nomogram models for predicting urinary incontinence following radical prostatectomy in high-risk prostate cancer patients.Am J Cancer Res. 2025 Jul 15;15(7):3017-3034. doi: 10.62347/ZYAA3728. eCollection 2025. Am J Cancer Res. 2025. PMID: 40814370 Free PMC article.
References
-
- Mottet N, van den Bergh RCN, Briers E, Van den Broeck T, Cumberbatch MG, De Santis M et al (2021) EAU-EANM-ESTRO-ESUR-SIOG guidelines on prostate cancer—2020 update. Part 1: screening, diagnosis, and local treatment with curative intent. Eur Urol 79:243–262. 10.1016/j.eururo.2020.09.042 - PubMed
-
- Fanshawe JB, Wai-Shun Chan V, Asif A, Ng A, Van Hemelrijck M, Cathcart P et al (2023) Decision regret in patients with localised prostate cancer: a systematic review and meta-analysis. Eur Urol Oncol. 10.1016/j.euo.2023.02.005 - PubMed
-
- Ficarra V, Novara G, Rosen RC, Artibani W, Carroll PR, Costello A et al (2012) Systematic review and meta-analysis of studies reporting urinary continence recovery after robot-assisted radical prostatectomy. Eur Urol 62:405–417. 10.1016/j.eururo.2012.05.045 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
