

An international phantom study of inter-site variability in Technetium-99m image quantification: analyses from the TARGET radioembolization study
- PMID: 38809320
- PMCID: PMC11136909
- DOI: 10.1186/s40658-024-00647-x
An international phantom study of inter-site variability in Technetium-99m image quantification: analyses from the TARGET radioembolization study
Abstract
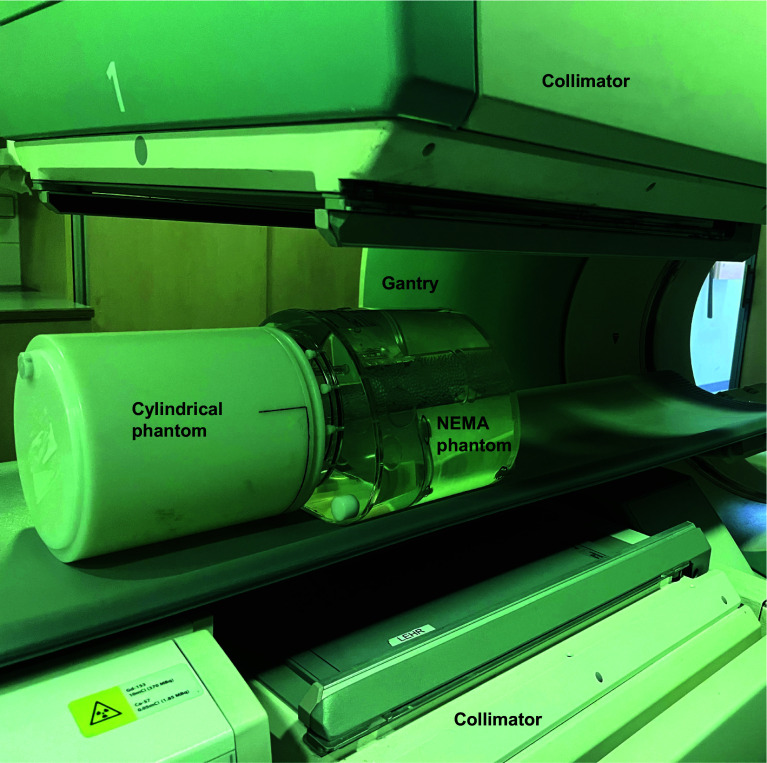
Background: Personalised multi-compartment dosimetry based on [99mTc]Tc-MAA is a valuable tool for planning 90Y radioembolization treatments. The establishment and effective application of dose-effect relationships in yttrium-90 (90Y) radioembolization requires [99mTc]Tc-MAA SPECT quantification ideally independent of clinical site. The purpose of this multi-centre phantom study was to evaluate inter-site variability of [99mTc]Tc-MAA imaging and evaluate a standardised imaging protocol. Data was obtained from the TARGET study, an international, retrospective multi-centre study including 14 sites across 8 countries. The impact of imaging related factors was estimated using a NEMA IQ phantom (representing the liver), and a uniformly filled cylindrical phantom (representing the lungs). Imaging was performed using site-specific protocols and a standardized protocol. In addition, the impact of implementing key image corrections (scatter and attenuation correction) in the site-specific protocols was investigated. Inter-site dosimetry accuracy was evaluated by comparing computed Lung Shunt Fraction (LSF) measured using planar imaging of the cylindrical and NEMA phantom, and contrast recovery coefficient (CRC) measured using SPECT imaging of the NEMA IQ phantom.
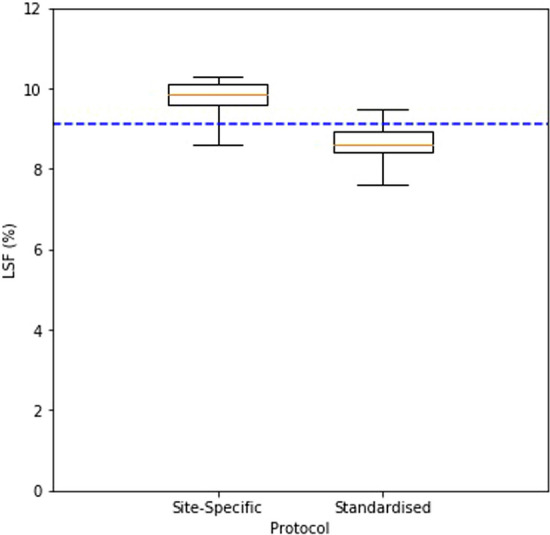
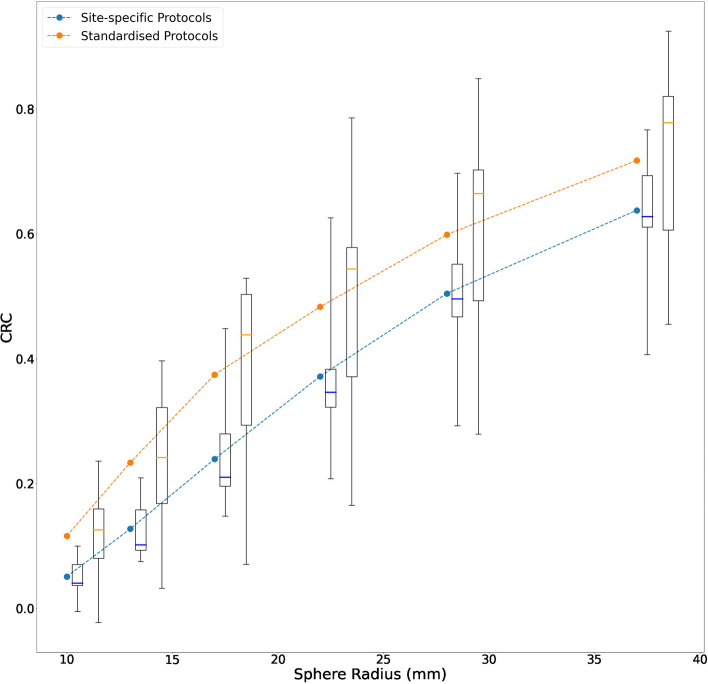
Results: Regarding the LSF, inter-site variation with planar site-specific protocols was minimal, as determined by comparing computed LSF between sites (interquartile range 9.6-10.1%). A standardised protocol did not improve variation (interquartile range 8.4-9.0%) but did improve mean accuracy compared to the site-specific protocols (5.0% error for standardised protocol vs 8.8% error for site-specific protocols). Regarding the CRC, inter-system variation was notable for site-specific SPECT protocols and could not be improved by the standardised protocol (CRC interquartile range for 37 mm sphere 0.5-0.7 and 0.6-0.8 respectively), however the standardised protocol did improve accuracy of sphere:background determination. Implementation of key image corrections did improve inter-site variation (CRC interquartile range for 37 mm sphere 0.6-0.7).
Conclusion: Eliminating sources of variability in image corrections between imaging protocols reduces inter-site variation in quantification. A standardised protocol was not able to improve consistency of LSF or CRC but was able to improve accuracy.
Keywords: Harmonization; Imaging; Macroaggregated-albumin (MAA); Performance; SPECT/CT; Technetium-99m; Yttrium-90.
© 2024. The Author(s).
Conflict of interest statement
Grace Keane, MSc (GK): Is a consultant for Boston Scientific. Rob van Rooij, PhD (RVR): Is a consultant for Boston Scientific and Quirem Medical. Marnix Lam, MD, PhD (ML): Is a consultant for Boston Scientific, Terumo and Quirem Medical. He receives research support from Boston Scientific, Terumo and Quirem Medical. Cheenu Kappadath, PhD (CK): Is a consultant for Boston Scientific, Sirtex Medicine and Terumo Medical. He receives research support from Boston Scientific, Sirtex Medical and Terumo Medical. Bilal Kovan, PhD (BK): none. Stephanie Leon, PhD (SL): none. Matthew Dreher, PhD (MD): Works for Boston Scientific. Kirk D. Fowers, PhD (KF): Works for Boston Scientific. Hugo de Jong, PhD (HDJ): Is a consultant for Boston Scientific and Quirem Medical.
Figures


Similar articles
-
The value of 99mTc-MAA SPECT/CT for lung shunt estimation in 90Y radioembolization: a phantom and patient study.EJNMMI Res. 2018 Jun 15;8(1):50. doi: 10.1186/s13550-018-0402-8. EJNMMI Res. 2018. PMID: 29904808 Free PMC article.
-
Hepatopulmonary Shunt Ratio Verification Model for Transarterial Radioembolization.Curr Radiopharm. 2024;17(3):276-284. doi: 10.2174/0118744710284130240108053733. Curr Radiopharm. 2024. PMID: 38288829
-
Radioembolization lung shunt estimation based on a 90 Y pretreatment procedure: A phantom study.Med Phys. 2018 Oct;45(10):4744-4753. doi: 10.1002/mp.13168. Epub 2018 Sep 21. Med Phys. 2018. PMID: 30179259
-
Feasibility of imaging 90 Y microspheres at diagnostic activity levels for hepatic radioembolization treatment planning.Med Phys. 2020 Mar;47(3):1105-1114. doi: 10.1002/mp.13974. Epub 2020 Jan 20. Med Phys. 2020. PMID: 31855282 Free PMC article.
-
Calculation of lung mean dose and quantification of error for 90 Y-microsphere radioembolization using 99m Tc-MAA SPECT/CT and diagnostic chest CT.Med Phys. 2019 Sep;46(9):3929-3940. doi: 10.1002/mp.13575. Epub 2019 Jun 11. Med Phys. 2019. PMID: 31063600
References
-
- Garin E, Rolland Y, Pracht M, Le Sourd S, Laffont S, Mesbah H, et al. High impact of macroaggregated albumin-based tumour dose on response and overall survival in hepatocellular carcinoma patients treated with (90) Y-loaded glass microsphere radioembolization. Liver Int. 2017;37:101–110. doi: 10.1111/liv.13220. - DOI - PMC - PubMed
-
- Chiesa C, Mira M, Maccauro M, Romito R, Spreafico C, Sposito C, et al. A dosimetric treatment planning strategy in radioembolization of hepatocarcinoma with 90Y glass microspheres. Q J Nucl Med Mol Imaging. 2012;56:503–508. - PubMed
-
- Garin E, Tselikas L, Guiu B, Chalaye J, Edeline J, de Baere T, et al. Personalised versus standard dosimetry approach of selective internal radiation therapy in patients with locally advanced hepatocellular carcinoma (DOSISPHERE-01): a randomised, multicentre, open-label phase 2 trial. Lancet Gastroenterol Hepatol. 2021;6:17–29. doi: 10.1016/s2468-1253(20)30290-9. - DOI - PubMed
LinkOut - more resources
Full Text Sources
