

Inflammatory Markers in Prior Loop Electrosurgical Excision Procedure (LEEP) as a Prognosis Factor in the Recurrence of Cervical Intraepithelial Neoplasia
- PMID: 38809635
- PMCID: PMC11318804
- DOI: 10.31557/APJCP.2024.25.5.1635
Inflammatory Markers in Prior Loop Electrosurgical Excision Procedure (LEEP) as a Prognosis Factor in the Recurrence of Cervical Intraepithelial Neoplasia
Abstract
Objectives: To investigate the relationship between preoperative inflammatory markers and recurrence of CIN after loop electrosurgical excision procedure (LEEP).
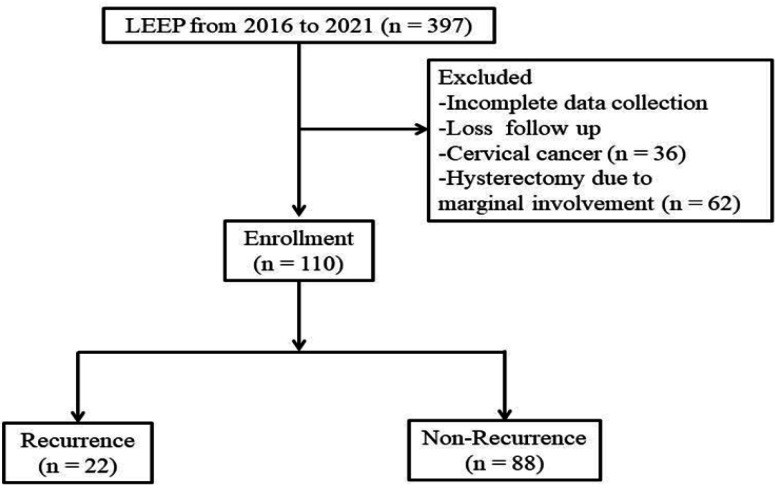
Methods: A retrospective historical cohort study was conducted at gynecologic oncology unit, Bhumibol Adulyadej Hospital, Royal Thai Air Force, Thailand. Data was collected from medical records of CIN cases from year 2016 to 2021. Inclusion criteria were subjects who were diagnosed of CIN and underwent LEEP with pathologic confirmation and followed up for two years (at 6 months, 1 year, and 2 years). Preoperative complete blood count (CBC) was obtained within one month for calculation as systemic inflammatory values.
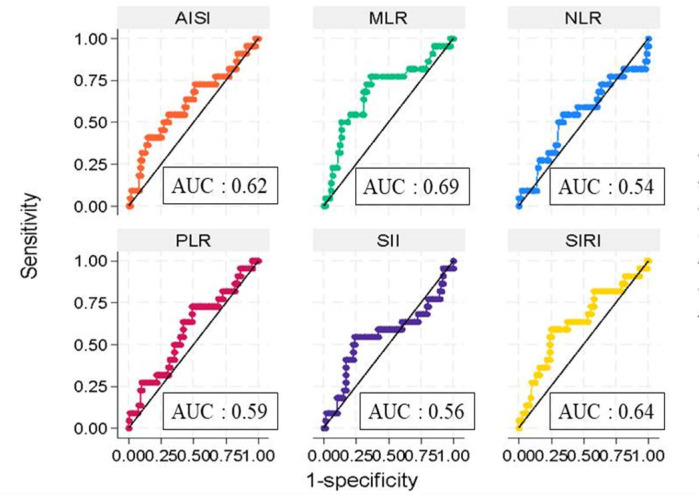
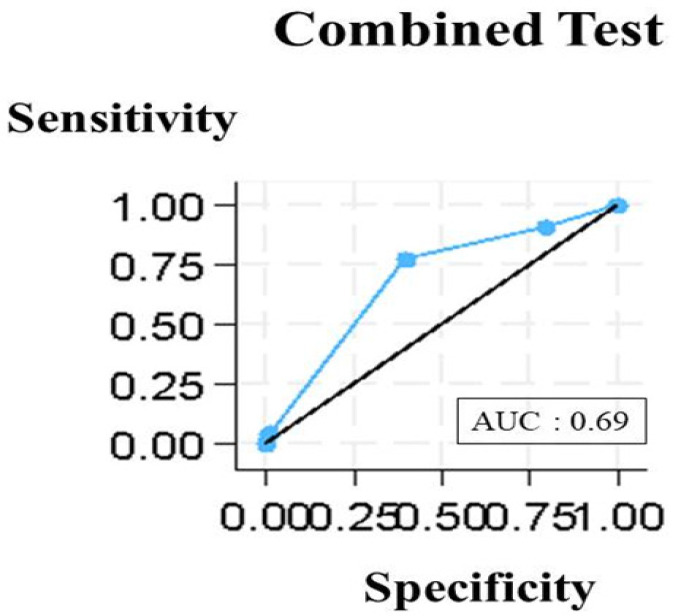
Results: One hundred and ten cases of CIN were enrolled. Mean age of participants was 48.1 years old. Three-fourths (83/110) of the participants had histological confirmation as CIN2/3. Sixteen (18/110) and twenty (22/110) percentage of cases had recurrence of disease at 1 and 2 years, respectively. Monocytes /lymphocytes ratio (MLR) and systemic inflammation response index (SIRI) could predict recurrence of CIN within 2 years. MLR more than 0.16 and SIRI more than 0.57 gave the sensitivity and negative predictive value (NPV) at percentage of 77.3/ 81.8 and 91.8/ 90.2, respectively. Combination of MLR and SIRI had sensitivity and NPV at 90.5 and 95.4 percent, respectively. MLR and SIRI could not predict marginal involvement, glandular involvement, and LEEP confirmed CIN 2/3.
Conclusion: Pretreatment MLR and SIRI were statistically significant in predicting the recurrence in CIN after post LEEP procedure within 2 years follow up.
Keywords: Keywords: CIN; MLR; SIRI; recurrent.
Conflict of interest statement
The authors declares that there is no conflict of interest.
Figures
References
-
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: Globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–49. - PubMed
-
- World Health Organization. WHO guidelines for the use of thermal ablation for cervical pre-cancer lesions. Geneva: World Health Organization; 2019. - PubMed