

Comparison of quantitative radiomorphometric predictors of healthy and MRONJ-affected bone using panoramic radiography and cone-beam CT
- PMID: 38810135
- PMCID: PMC11358619
- DOI: 10.1093/dmfr/twae024
Comparison of quantitative radiomorphometric predictors of healthy and MRONJ-affected bone using panoramic radiography and cone-beam CT
Abstract
Objectives: To determine the most distinctive quantitative radiomorphometric parameter(s) for the detection of MRONJ-affected bone changes in panoramic radiography (PR) and cone-beam CT (CBCT).
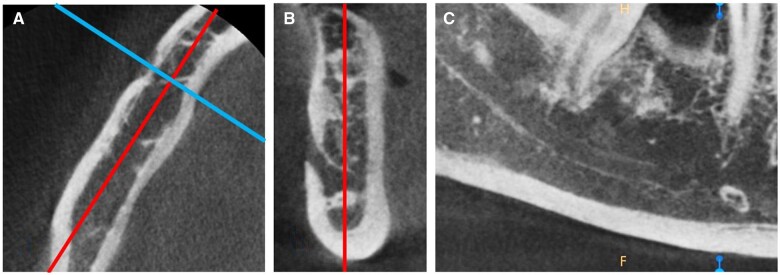
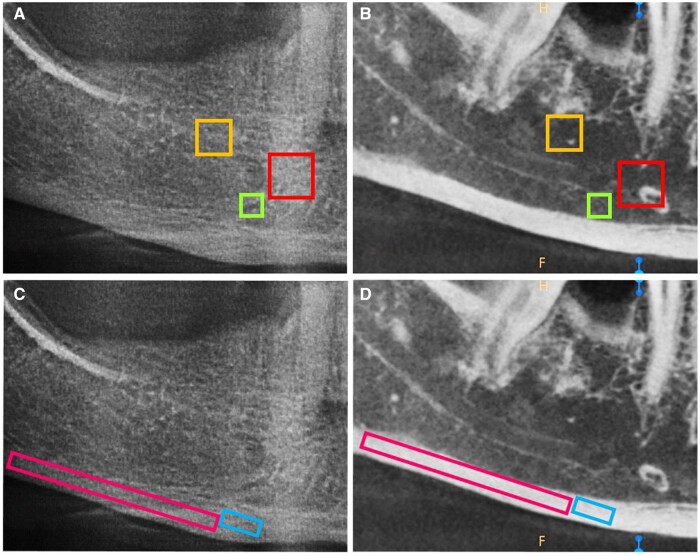
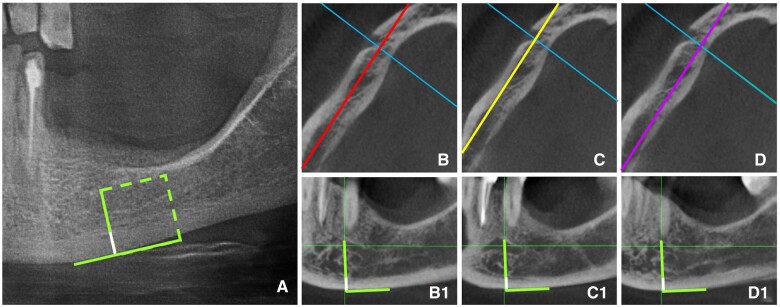
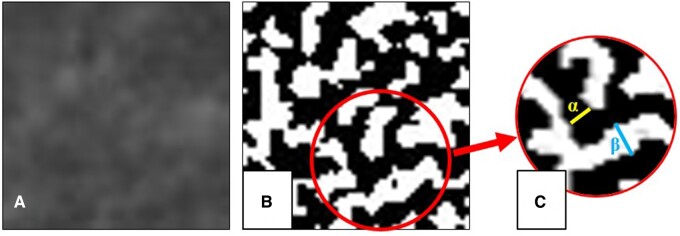
Methods: PR and sagittal CBCT slices of 24 MRONJ patients and 22 healthy controls were used for the measurements of mandibular cortical thickness (MCT), fractal dimension (FD), lacunarity, mean gray value (MGV), bone area fraction (BA/TA), trabecular thickness (Tb.Th), trabecular separation (Tb.Sp), trabecular number (Tb.N). MCT was measured in the mental foramen region. While FD and lacunarity were measured on mandibular trabecular and cortical regions-of-interest (ROIs), the remaining parameters were measured on trabecular ROIs. The independent samples t-test was used to compare the measurements between the MRONJ and control groups for both imaging modalities (P = .05).
Results: MCT was the only parameter that differentiated MRONJ-affected bone in both PR and CBCT (P < .05). None of the remaining parameters revealed any difference for MRONJ-affected bone in CBCT (P > .05). FD, lacunarity, MGV, BA/TA, and Tb.Sp could distinguish MRONJ-affected trabecular bone in PR (P < .05). The correspondent ROI for both imaging methods that was reliable for detecting MRONJ-affected bone was the trabecular bone distal to the mental foramen above the inferior alveolar canal (ROI-3).
Conclusions: MCT is a reliable parameter for the discrimination of MRONJ-affected bone in both PR and CBCT images. PR may be used to detect MRONJ-affected trabecular bone using FD, lacunarity, MGV, BA/TA, and Tb.Sp measurements as well.
Keywords: cone-beam CT; medication-related osteonecrosis of the jaws; panoramic radiography; quantitative bone parameters.
© The Author(s) 2024. Published by Oxford University Press on behalf of the British Institute of Radiology and the International Association of Dentomaxillofacial Radiology.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
Similar articles
-
Evaluation of trabecular pattern of mandible using fractal dimension, bone area fraction, and gray scale value: comparison of cone-beam computed tomography and panoramic radiography.Oral Radiol. 2019 Jan;35(1):35-42. doi: 10.1007/s11282-018-0316-1. Epub 2018 Jan 17. Oral Radiol. 2019. PMID: 30484179
-
Fractal dimension, lacunarity, and bone area fraction analysis of peri-implant trabecular bone after prosthodontic loading.Oral Radiol. 2025 Jan;41(1):120-130. doi: 10.1007/s11282-024-00784-0. Epub 2024 Nov 11. Oral Radiol. 2025. PMID: 39523226
-
Fractal Dimension and Lacunarity Analysis in the Dentulous and Edentulous Mandibular Posterior Region Using Cone-beam Computed Tomography: A Cross-sectional Retrospective Study.J Contemp Dent Pract. 2024 Jun 1;25(6):581-587. doi: 10.5005/jp-journals-10024-3701. J Contemp Dent Pract. 2024. PMID: 39364825
-
Medication-Related Osteonecrosis of the Jaw-Comparison of Bone Imaging Using Ultrashort Echo-Time Magnetic Resonance Imaging and Cone-Beam Computed Tomography.Invest Radiol. 2020 Mar;55(3):160-167. doi: 10.1097/RLI.0000000000000617. Invest Radiol. 2020. PMID: 31688157 Clinical Trial.
-
Do various imaging modalities provide potential early detection and diagnosis of medication-related osteonecrosis of the jaw? A review.Dentomaxillofac Radiol. 2021 Sep 1;50(6):20200417. doi: 10.1259/dmfr.20200417. Epub 2021 Jan 15. Dentomaxillofac Radiol. 2021. PMID: 33411572 Free PMC article. Review.
Cited by
-
Bone-formation-related markers in osteonecrosis of the jaws and their correlation with radiographic findings.Oral Maxillofac Surg. 2025 Aug 11;29(1):140. doi: 10.1007/s10006-025-01439-y. Oral Maxillofac Surg. 2025. PMID: 40784978
References
-
- Ruggiero SL, Dodson TB, Aghaloo T, Carlson ER, Ward BB, Kademani D.. American Association of Oral and Maxillofacial Surgeons’ position paper on medication-related osteonecrosis of the jaws-2022 update. J Oral Maxillofac Surg. 2022;80(5):920-943. - PubMed
-
- Khan A, Morrison A, Cheung A, Hashem W, Compston J.. Osteonecrosis of the jaw (ONJ): diagnosis and management in 2015. Osteoporos Int. 2016;27(3):853-859. - PubMed
-
- Khosla S, Burr D, Cauley J, et al.Bisphosphonate-associated osteonecrosis of the jaw: report of a task force of the American Society for Bone and Mineral Research. J Bone Miner Res. 2007;22(10):1479-1491. - PubMed
-
- Torres SR, Chen CSK, Leroux BG, et al.Mandibular cortical bone evaluation on cone beam computed tomography images of patients with bisphosphonate-related osteonecrosis of the jaw. Oral Surg Oral Med Oral Pathol Oral Radiol. 2012;113(5):695-703. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
