

A systematic review of shared decision making training programs for general practitioners
- PMID: 38811922
- PMCID: PMC11137915
- DOI: 10.1186/s12909-024-05557-1
A systematic review of shared decision making training programs for general practitioners
Abstract
Background: Shared decision making (SDM) has been presented as the preferred approach for decisions where there is more than one acceptable option and has been identified a priority feature of high-quality patient-centered care. Considering the foundation of trust between general practitioners (GPs) and patients and the variety of diseases in primary care, the primary care context can be viewed as roots of SDM. GPs are requesting training programs to improve their SDM skills leading to a more patient-centered care approach. Because of the high number of training programs available, it is important to overview these training interventions specifically for primary care and to explore how these training programs are evaluated.
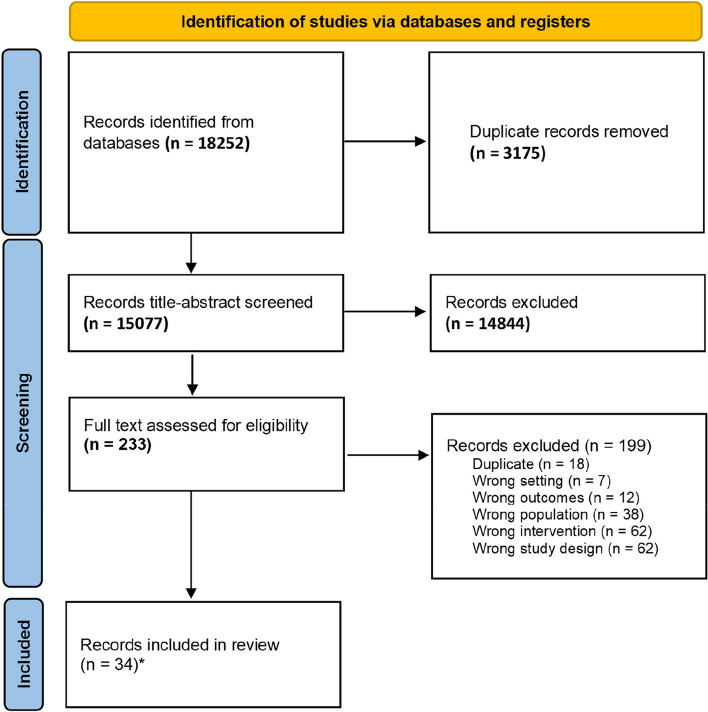
Methods: This review was reported in accordance with the PRISMA guideline. Eight different databases were used in December 2022 and updated in September 2023. Risk of bias was assessed using ICROMS. Training effectiveness was analyzed using the Kirkpatrick evaluation model and categorized according to training format (online, live or blended learning).
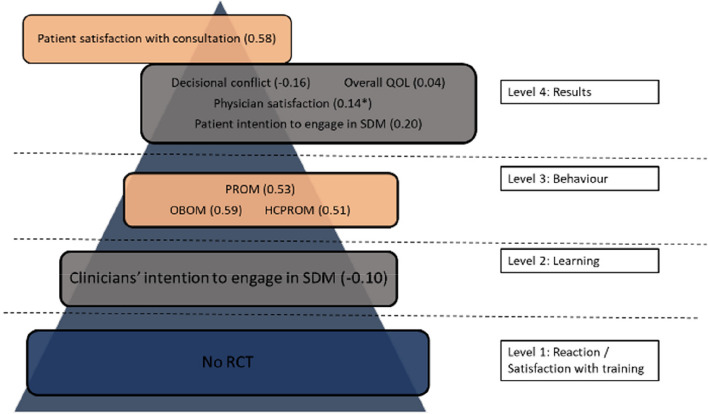
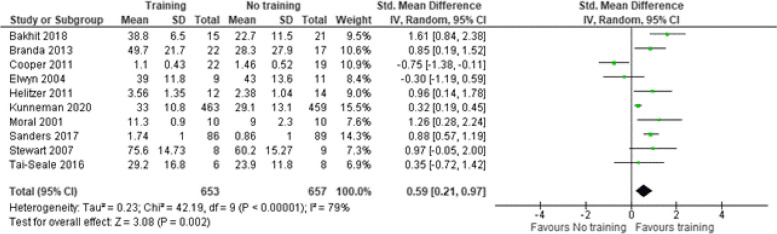
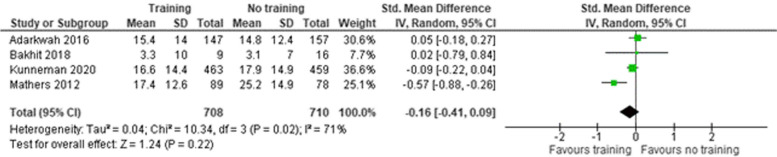
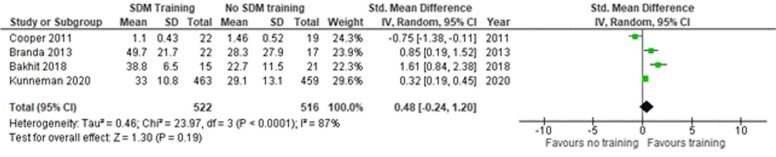
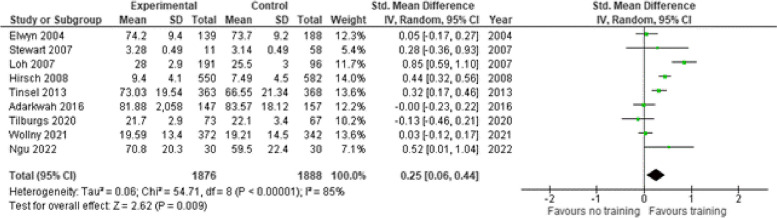
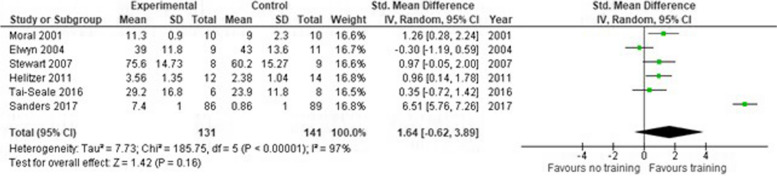
Results: We identified 29 different SDM training programs for GPs. SDM training has a moderate impact on patient (SMD 0.53 95% CI 0.15-0.90) and observer reported SDM skills (SMD 0.59 95%CI 0.21-0.97). For blended training programs, we found a high impact for quality of life (SMD 1.20 95% CI -0.38-2.78) and patient reported SDM skills (SMD 2.89 95%CI -0.55-6.32).
Conclusion: SDM training improves patient and observer reported SDM skills in GPs. Blended learning as learning format for SDM appears to show better effects on learning outcomes than online or live learning formats. This suggests that teaching facilities designing SDM training may want to prioritize blended learning formats. More homogeneity in SDM measurement scales and evaluation approaches and direct comparisons of different types of educational formats are needed to develop the most appropriate and effective SDM training format.
Trial registration: PROSPERO: A systematic review of shared-decision making training programs in a primary care setting. PROSPERO 2023 CRD42023393385 Available from: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42023393385 .
Keywords: Decision making; Educational intervention; General practitioner; Shared decision making.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures








References
-
- Kramer P, Damhuis E, Verhue D. Samen Beslissen: Doelgroepenonderzoek onder zorgverleners en zorggebruikers. Campagne Samen Beslissen in de Zorg. Programma Uitkomstgerichte Zorg. The Netherlands: KANTAR; 2022. p. 5–79. https://demedischspecialist.nl/sites/default/files/2022-10/rapport_campa....
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
