

Molecular classification and biomarkers of outcome with immunotherapy in extensive-stage small-cell lung cancer: analyses of the CASPIAN phase 3 study
- PMID: 38811992
- PMCID: PMC11137956
- DOI: 10.1186/s12943-024-02014-x
Molecular classification and biomarkers of outcome with immunotherapy in extensive-stage small-cell lung cancer: analyses of the CASPIAN phase 3 study
Abstract
Background: We explored potential predictive biomarkers of immunotherapy response in patients with extensive-stage small-cell lung cancer (ES-SCLC) treated with durvalumab (D) + tremelimumab (T) + etoposide-platinum (EP), D + EP, or EP in the randomized phase 3 CASPIAN trial.
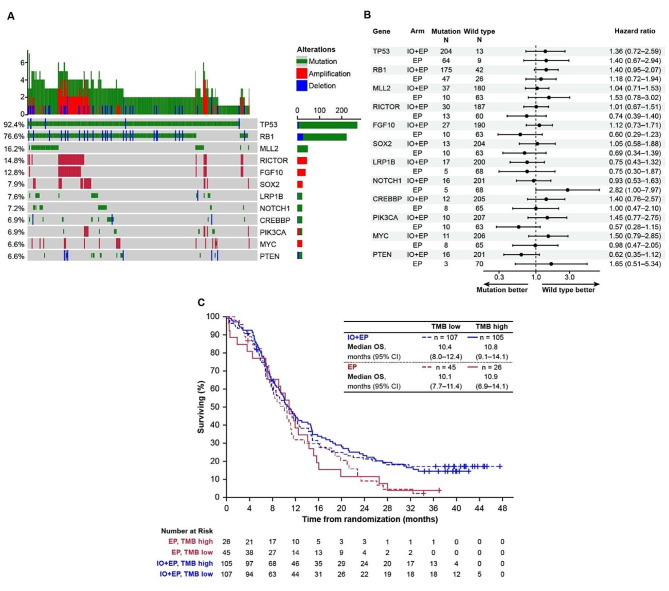
Methods: 805 treatment-naïve patients with ES-SCLC were randomized (1:1:1) to receive D + T + EP, D + EP, or EP. The primary endpoint was overall survival (OS). Patients were required to provide an archived tumor tissue block (or ≥ 15 newly cut unstained slides) at screening, if these samples existed. After assessment for programmed cell death ligand-1 expression and tissue tumor mutational burden, residual tissue was used for additional molecular profiling including by RNA sequencing and immunohistochemistry.
Results: In 182 patients with transcriptional molecular subtyping, OS with D ± T + EP was numerically highest in the SCLC-inflamed subtype (n = 10, median 24.0 months). Patients derived benefit from immunotherapy across subtypes; thus, additional biomarkers were investigated. OS benefit with D ± T + EP versus EP was greater with high versus low CD8A expression/CD8 cell density by immunohistochemistry, but with no additional benefit with D + T + EP versus D + EP. OS benefit with D + T + EP versus D + EP was associated with high expression of CD4 (median 25.9 vs. 11.4 months) and antigen-presenting and processing machinery (25.9 vs. 14.6 months) and MHC I and II (23.6 vs. 17.3 months) gene signatures, and with higher MHC I expression by immunohistochemistry.
Conclusions: These findings demonstrate the tumor microenvironment is important in mediating better outcomes with D ± T + EP in ES-SCLC, with canonical immune markers associated with hypothesized immunotherapy mechanisms of action defining patient subsets that respond to D ± T.
Trial registration: ClinicalTrials.gov, NCT03043872.
Keywords: Antigen presentation machinery; Biomarkers; CTLA-4; Gene expression profiling; Molecular subtyping; PD-L1; SCLC subtypes; Small-cell lung cancer; T-cell inflamed signature.
© 2024. The Author(s).
Conflict of interest statement
M.X., M.V., J.R.-C., J.Z., M.S., H.J., J.C.B., R.A.S., Z.L., and Y.S. are/were employees of AstraZeneca and may own stock or stock options. C.O’B. is a contractor for AstraZeneca. L.P.-A. has served on advisory councils or committees for Altum Sequencing and Stab Therapeutics, has received honoraria from AstraZeneca, Janssen, Merck, and Mirati, has received consulting fees from Eli Lilly, MSD, Roche, Pharmamar, Merck KgaA (Darmstadt, Germany), AstraZeneca, Novartis, Servier, Amgen, Pfizer, Bayer, Bristol-Myers Squibb, Mirati, GlaxoSmithKline, Janssen, Takeda, Regeneron, and Sanofi, and has received grants or funds from MSD, AstraZeneca, Bristol-Myers Squibb, Pfizer, and Pharmamar. J.W.G. reports research grants from AbbVie, AstraZeneca, Bristol-Myers Squibb, Genentech, and Merck, consulting fees from AbbVie, AstraZeneca, Bristol-Myers Squibb, and Genentech, and support for travel from AstraZeneca. M.C.G. discloses competing financial interests with MSD Oncology, AstraZeneca/MedImmune, GlaxoSmithKline, Takeda, Roche, Bristol-Myers Squibb, Daiichi-Sankyo/AstraZeneca, Regeneron, Pfizer, Blueprint Medicines, Novartis, Sanofi-Aventis, and Medscape; holds advisory/management and consulting positions with Bristol-Myers Squibb, MSD, AstraZeneca, Novartis, Takeda, Roche, Sanofi-Aventis, Celgene, Daiichi-Sankyo, Pfizer, Seattle Genetics, Eli Lilly, GlaxoSmithKline, Bayer Healthcare Pharmaceuticals, Blueprint Medicines, Janssen, Regeneron, Bayer, AbbVie, Mirati, Merck, Boheringer Ingelheim, Blueprint Medicines, and Abion; is a member of a speakers bureau for AstraZeneca, MSD Oncology, Merck, Mirati, and Daiichi-Sankyo/AstraZeneca; and has received institutional research funding from Bristol-Myers Squibb, MSD, Roche/Genentech, AstraZeneca/MedImmune, AstraZeneca, Pfizer, GlaxoSmithKline, Novartis, Merck, Incyte, Takeda, Spectrum Pharmaceuticals, Blueprint Medicines, Eli Lilly, Ipsen, Janssen, Exelixis, MedImmune, Sanofi, and Amgen. C.M.G. discloses advisory/management and consulting positions with AstraZeneca, Bristol-Myers Squibb, Catalyst, Daiichi-Sankyo, G1 Therapeutics, Jazz Pharmaceuticals, Monte Rosa, and STCube; and holds Patent No. 11, 732, 306 (Molecular subtyping of small cell lung cancer to predict therapeutic responses). J.V.H. discloses scientific advisory boards for AstraZeneca and Genentech; patent applications pending on SCLC classification; research funding from AstraZeneca; and that MD Anderson has licensing agreements with Nucleix and BostonGene for the development of biomarkers for SCLC subgroups. L.A.B. discloses advisory/management and consulting positions with MSD, Arrowhead Pharmaceuticals, Chugai Pharmaceutical Co., AstraZeneca, Genentech, BeiGene, AbbVie, Jazz Pharmaceuticals, Puma Biotechnology, Amgen, and Daiichi-Sankyo; and holds Patent No. 11, 732, 306 (Molecular subtyping of small cell lung cancer to predict therapeutic responses). C.M.R. has consulted regarding oncology drug development with AbbVie, Amgen, AstraZeneca, D2G, Daiichi-Sankyo, Epizyme, Genentech/Roche, Ipsen, Jazz, Kowa, Eli Lilly, Merck, and Syros; and serves on the scientific advisory boards of Auron, Bridge Medicines, DISCO, Earli, and Harpoon Therapeutics.
Figures





References
-
- Gay CM, Stewart CA, Park EM, Diao L, Groves SM, Heeke S, et al. Patterns of transcription factor programs and immune pathway activation define four major subtypes of SCLC with distinct therapeutic vulnerabilities. Cancer Cell. 2021;39:346–e360347. doi: 10.1016/j.ccell.2020.12.014. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
