

A multicenter, matched case-control analysis comparing burden of illness among patients with tuberous sclerosis complex related epilepsy, generalized idiopathic epilepsy, and focal epilepsy in Germany
- PMID: 38812055
- PMCID: PMC11138101
- DOI: 10.1186/s42466-024-00323-6
A multicenter, matched case-control analysis comparing burden of illness among patients with tuberous sclerosis complex related epilepsy, generalized idiopathic epilepsy, and focal epilepsy in Germany
Abstract
Background: Depending on the underlying etiology and epilepsy type, the burden of disease for patients with seizures can vary significantly. This analysis aimed to compare direct and indirect costs and quality of life (QoL) among adults with tuberous sclerosis complex (TSC) related with epilepsy, idiopathic generalized epilepsy (IGE), and focal epilepsy (FE) in Germany.
Methods: Questionnaire responses from 92 patients with TSC and epilepsy were matched by age and gender, with responses from 92 patients with IGE and 92 patients with FE collected in independent studies. Comparisons were made across the main QoL components, direct costs (patient visits, medication usage, medical equipment, diagnostic procedures, ancillary treatments, and transport costs), indirect costs (employment, reduced working hours, missed days), and care level costs.
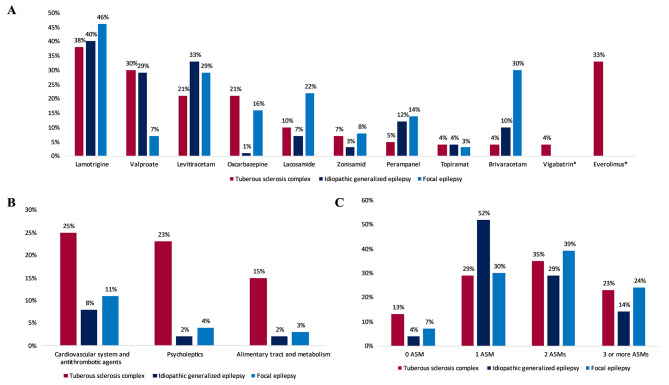
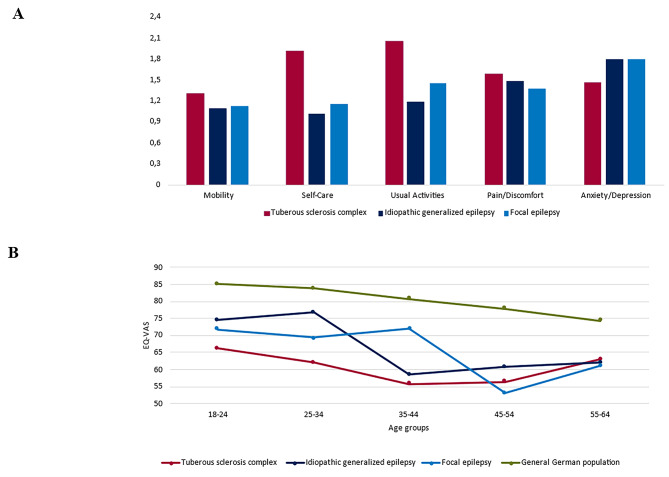
Results: Across all three cohorts, mean total direct costs (TSC: €7602 [median €2620]; IGE: €1919 [median €446], P < 0.001; FE: €2598 [median €892], P < 0.001) and mean total indirect costs due to lost productivity over 3 months (TSC: €7185 [median €11,925]; IGE: €3599 [median €0], P < 0.001; FE: €5082 [median €2981], P = 0.03) were highest among patients with TSC. The proportion of patients with TSC who were unemployed (60%) was significantly larger than the proportions of patients with IGE (23%, P < 0.001) or FE (34%, P = P < 0.001) who were unemployed. Index scores for the EuroQuol Scale with 5 dimensions and 3 levels were significantly lower for patients with TSC (time-trade-off [TTO]: 0.705, visual analog scale [VAS]: 0.577) than for patients with IGE (TTO: 0.897, VAS: 0.813; P < 0.001) or FE (TTO: 0.879, VAS: 0.769; P < 0.001). Revised Epilepsy Stigma Scale scores were also significantly higher for patients with TSC (3.97) than for patients with IGE (1.48, P < 0.001) or FE (2.45, P < 0.001). Overall Quality of Life in Epilepsy Inventory-31 items scores was significantly lower among patients with TSC (57.7) and FE (57.6) than among patients with IGE (66.6, P = 0.004 in both comparisons). Significant differences between patients with TSC and IGE were also determined for Neurological Disorder Depression Inventory for Epilepsy (TSC: 13.1; IGE: 11.2, P = 0.009) and Liverpool Adverse Events Profile scores (TSC: 42.7; IGE: 37.5, P = 0.017) with higher score and worse results for TSC patients in both questionnaires.
Conclusions: This study is the first to compare patients with TSC, IGE, and FE in Germany and underlines the excessive QoL burden and both direct and indirect cost burdens experienced by patients with TSC.
Keywords: Anti-seizure medication; Anticonvulsants; Costs; Depression; Direct costs; Everolimus; Indirects costs; Quality of life; Seizure; Stigma.
© 2024. The Author(s).
Conflict of interest statement
LL and none of the other authors report conflicts of interest related to this study.
CH reports personal fees from Desitin Arzneimittel, Eisai, GW Pharmaceuticals companies, Novartis, Shire, and Zogenix.
SKn received speaker´s honoraria from Angelini Pharma, Bial, Desitin Arzneimittel, Eisai, Epliog, GW Pharmaceuticals, Kanso, UCB Pharma, and Zogenix.
MK does not have any COI. He receives no honoraria from pharmaceutical companies.
FvP reports personal fees and grants from Bial, Desitin Arzneimittel, Eisai, GW Pharmaceutical companies, Arvelle Therapeutics, Zogenix, and UCB Pharma.
LW does not have any COI. He receives no honoraria from pharmaceutical companies.
SKo reports speakers honoraria from Eisai, UCB and Jazz Pharma, and research funding from Biogen.
JPZ does not have any COI. He receives no honoraria from pharmaceutical companies.
MS reports personal fees from Novartis and GW Pharmaceuticals companies.
GKu reports honoraria for speaking engagements from Desitin Arzneimittel, Eisai, UCB Pharma, Takeda, Shire, Zogenix, Neuraxpharm, Stada, and GW Pharmaceuticals.
TM does not have any COI. He receives no honoraria from pharmaceutical companies.
AB reports grants from UCB Pharma and honoraria for speaking engagements from Biogen, Desitin Arzneimittel, Eisai GmbH, GW Pharmaceuticals, Neuraxpharm, Shire/Takeda GmbH, UCB Pharma, and ViroPharma.
KM does not have any COI. He receives no honoraria from pharmaceutical companies.
SM reports grants from Novartis, UCB, Shire, Deutsche Forschungsgemeinschaft und Epilepsiestiftung Dr. Wolf.
HS does not have any COI. She receives no honoraria from pharmaceutical companies.
CT does not have any COI. She receives no honoraria from pharmaceutical companies.
BZ does not have any COI. She receives no honoraria from pharmaceutical companies.
SSB reports personal fees from Eisai, Desitin Pharma, GW Pharmaceuticals, Zogenix, UCB Pharma, and Marinus Pharma.
JPR does not have any COI. He receives no honoraria from pharmaceutical companies.
FR reports personal fees from Angelini Pharma, Eisai, Jazz Pharma, and UCB Pharma and grants from the Detlev-Wrobel-Fonds for Epilepsy Research, the Deutsche Forschungsgemeinschaft (DFG), the Federal Ministry of Education and Research (BMBF), the LOEWE Programme of the State of Hesse, and the European Union. FR reports that he is part of the editorial board of Neurological Research and Practice.
AS reports personal fees and grants from Angelini Pharma, Biocodex, Desitin Arzneimittel, Eisai, Jazz Pharmaceuticals, Marinus Pharma, Precisis, Takeda, UCB Pharma, and UNEEG Medical. AS reports that he is part of the editorial board of Neurological Research and Practice.
Figures

References
-
- Ebrahimi-Fakhari D, Mann LL, Poryo M, Graf N, von Kries R, Heinrich B, et al. Incidence of tuberous sclerosis and age at first diagnosis: New data and emerging trends from a national, prospective surveillance study. Orphanet Journal of Rare Diseases. 2018;13(1):117. doi: 10.1186/s13023-018-0870-y. - DOI - PMC - PubMed
-
- Dorn, T. (2022). Tuberous sclerosis complex (TSC). Zeitschrift für Epileptologie, 35(3), 242–249. 10.1007/s10309-022-00512-w
LinkOut - more resources
Full Text Sources