

A Descriptive Study on the Clinical Profile and Outcomes of Patients with COVID-19 and Tuberculosis Co-infection
- PMID: 38812770
- PMCID: PMC11132287
- DOI: 10.47895/amp.vi0.7855
A Descriptive Study on the Clinical Profile and Outcomes of Patients with COVID-19 and Tuberculosis Co-infection
Abstract
Background: Tuberculosis (TB) control has been a challenge in the country and its overall health impact remains significant. COVID-19 has caused significant morbidity and mortality especially among hospitalized patients. TB and COVID-19 co-infection (COVID-TB) may cause more catastrophic consequences and outcomes among afflicted individuals and management may be daunting. There is limited local data on COVID-TB.
Objectives: The clinical profile of COVID-TB patients who were admitted were described. Comparison of the clinical outcomes was also done versus the general admitted COVID-19 patients without concomitant TB in the same institution. Relevant patient outcomes were reported which included admission to an intensive care unit (ICU), length of hospital stay, and mortality rate.
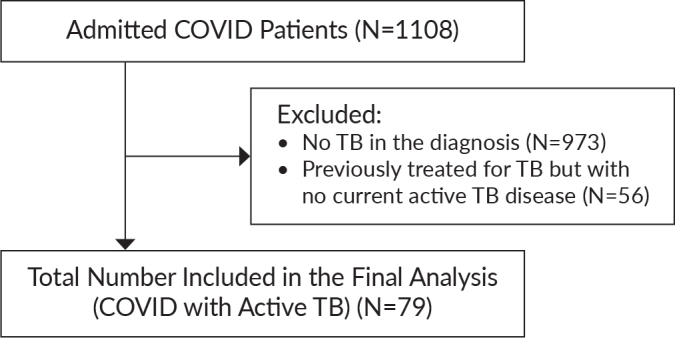
Methods: This is a descriptive study on the demographics and clinical outcomes of patients admitted in the Philippine General Hospital (PGH) for COVID-19 with TB co-infection from March 2020 to September 2020. We aimed to characterize patients with COVID-TB and analyzed their outcomes.
Results: There was a total of 79 patients who were admitted for COVID-19 (confirmed with RT-PCR) with TB co-infection during the study period. Majority of them were males (70.9%) with a median age of 54 (IQR 42 to 64) years. In terms of TB affliction, 75 (94.9%) patients were identified to have pulmonary tuberculosis. Majority of patients had at least one co-morbid illness with hypertension (16.5%), diabetes mellitus (13.9%), and heart failure (11.4%) as the most common. Respiratory symptoms (dyspnea and cough) were the predominant presenting complaint during hospital admission. Majority of the patients were classified as severe (8 or 10.1%) and critical (36 or 45.57%) COVID-19 disease. Fifty-six (70.9%) were bacteriologically confirmed tuberculosis. Radiologic imaging studies revealed findings consistent with pulmonary tuberculosis in 70 (88.61%) through plain radiograph. Forty-seven underwent HRCT and 46 of these (97.8%) had findings suggestive of PTB. Overall, 61 patients (77%) subsequently required oxygen supplementation. The in-hospital mortality within the study population was 36.7% (29/79) in contrast to the general COVID patients admitted in the same period which revealed significantly less fatality at 17.5% (35/200). The length of hospital stay was found to be 21.1 days ± 14.75 days across all study patients, and with median of 20 days for surviving patients. TB treatment outcomes were tracked in the 50 surviving COVID-19 patients where cure was declared in 8/50 (16%) while 22/50 (44%) successfully completed their six-month treatment regimen.
Conclusions: This study of COVID-TB provides an initial evaluation of the potential association between active TB infection and COVID-19 severity and mortality. The data generated from this study may be a starting point to assess the interaction of these two diseases. Furthermore, bidirectional screening may be recommended even at hospitals' triage areas since both diseases may have similar presentations.
Keywords: COVID-19; co-infection; tuberculosis.
© 2024 Acta Medica Philippina.
Conflict of interest statement
All authors declared no conflicts of interest.
Figures
References
-
- World Health Organization . Global Tuberculosis Report 2022 [Internet]. 2022. [cited 2022 Oct]. Available from: https://www.who.int/tb/publications/global_report/en/.
LinkOut - more resources
Full Text Sources