

Radioactive iodine refractoriness in Middle Eastern differentiated thyroid cancer: clinical outcome and risk factor analysis
- PMID: 38812819
- PMCID: PMC11133532
- DOI: 10.3389/fendo.2024.1326976
Radioactive iodine refractoriness in Middle Eastern differentiated thyroid cancer: clinical outcome and risk factor analysis
Abstract
Background: Radioactive iodine refractory differentiated thyroid cancer (RAIR-DTC) has received increasing attention due to its poor prognosis. However, outcomes may vary among patients with RAIR-DTC. The role of clinico-pathological and molecular prognostic factors in survival remains controversial, resulting in difficulty in selecting patients for new targeted therapies. We assessed mortality rate and DTC-specific survival in Middle Eastern RAIR-DTC to identify prognostic factors associated with survival.
Methods: This single center, retrospective study enrolled 268 patients with RAIR-DTC. Mortality rate and DTC-specific survival were analyzed to identify prognostic factors related to survival. Univariate and multivariate analysis were performed using Cox proportional hazards model.
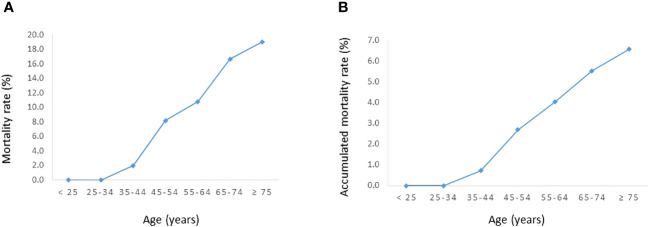
Results: Of the 268 cases of RAIR-DTC, 40.3% (108/268) had absent 131I uptake (either on diagnostic or post-therapy whole body scan), 15.3% (41/268) had progressive disease (PD) despite 131I, 7.5% (20/268) had persistent disease despite cumulative activity of I131 of >600 mCi and 36.9% (n=99/268) developed distant metastasis. On multivariate analysis, age (more than 45 years), presence of metastatic disease and tumors harboring telomerase reverse transcriptase (TERT) promoter mutations were independent prognostic factors for poor DTC-specific survival. Subjects were divided into 3 groups according to the number of risk factors; low risk (no risk factors); intermediate (≤ 2 risk factors); and high risk (all the 3 risk factors). Ten-year DTC-specific survival rates in low, intermediate and high-risk groups were 100.0%, 92.9% and 53.6%, respectively.
Conclusions: The contribution of age greater than 45 years to RAIR-DTC mortality is impactful. Older age, presence of distant metastasis and TERT mutations could be used as early predictors of RAIR-DTC cases. The identification of prognostic factors for poor survival in RAIR-DTC may improve the selection of patients for more personalized surveillance and therapeutic modalities.
Keywords: DTC-specific survival; TERT mutation; differentiated thyroid cancer; radioactive iodine refractory; risk factors.
Copyright © 2024 Parvathareddy, Siraj, Siraj, Ahmed, Al-Rasheed, Qadri, Siddiqui, Al-Sobhi, Al-Dayel and Al-Kuraya.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



Similar articles
-
TERT promoter mutations contribute to adverse clinical outcomes and poor prognosis in radioiodine refractory differentiated thyroid cancer.Sci Rep. 2024 Oct 10;14(1):23719. doi: 10.1038/s41598-024-75087-9. Sci Rep. 2024. PMID: 39390090 Free PMC article.
-
Clinical outcome and prognosis of differentiated thyroid carcinoma with distant metastasis.Nucl Med Commun. 2025 May 1;46(5):404-410. doi: 10.1097/MNM.0000000000001965. Epub 2025 Feb 27. Nucl Med Commun. 2025. PMID: 40013821
-
Clinicopathological features of differentiated thyroid carcinoma as predictors of the effects of radioactive iodine therapy.Ann Diagn Pathol. 2024 Apr;69:152243. doi: 10.1016/j.anndiagpath.2023.152243. Epub 2023 Dec 12. Ann Diagn Pathol. 2024. PMID: 38128440
-
Current Advances in Radioactive Iodine-Refractory Differentiated Thyroid Cancer.Curr Oncol. 2024 Jul 3;31(7):3870-3884. doi: 10.3390/curroncol31070286. Curr Oncol. 2024. PMID: 39057158 Free PMC article. Review.
-
Pathogenesis and signaling pathways related to iodine-refractory differentiated thyroid cancer.Front Endocrinol (Lausanne). 2024 Jan 19;14:1320044. doi: 10.3389/fendo.2023.1320044. eCollection 2023. Front Endocrinol (Lausanne). 2024. PMID: 38313845 Free PMC article. Review.
Cited by
-
Identifying risk factors associated with refractoriness to radioiodine therapy in differentiated thyroid cancer.Arch Endocrinol Metab. 2025 Aug 20;69(3):e250032. doi: 10.20945/2359-4292-2025-0032. Arch Endocrinol Metab. 2025. PMID: 40834361 Free PMC article.
-
Investigation into the Use of Surufatinib and Donafenib as Novel Multi-Kinase Inhibitors Therapeutic Agents in Managing Advanced Differentiated Thyroid Cancer: A Systematic Review.Biomedicines. 2025 Mar 20;13(3):752. doi: 10.3390/biomedicines13030752. Biomedicines. 2025. PMID: 40149728 Free PMC article. Review.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical