Novel parameters for predicting fluid responsiveness during the mini fluid challenge and ability of the cardiac power index: an observational cohort study
- PMID: 38813019
- PMCID: PMC10763793
- DOI: 10.55730/1300-0144.5688
Novel parameters for predicting fluid responsiveness during the mini fluid challenge and ability of the cardiac power index: an observational cohort study
Abstract
Background/aim: The percentage change in the stroke volume index (SVI) due to the mini fluid challenge (MFC) (MFC-ΔSVI%) is used commonly in daily practice. However, up to 20% of patients remain in the gray zone of this variable. Thus, it was aimed to compare the MFC-ΔSVI% and the percentage change in the cardiac power index (CPI) due to the MFC (MFC-ΔCPI%) with the baseline values of the pulse pressure variation (PPV) and stroke volume variation (SVV) in terms of their abilities to predict fluid responsiveness.
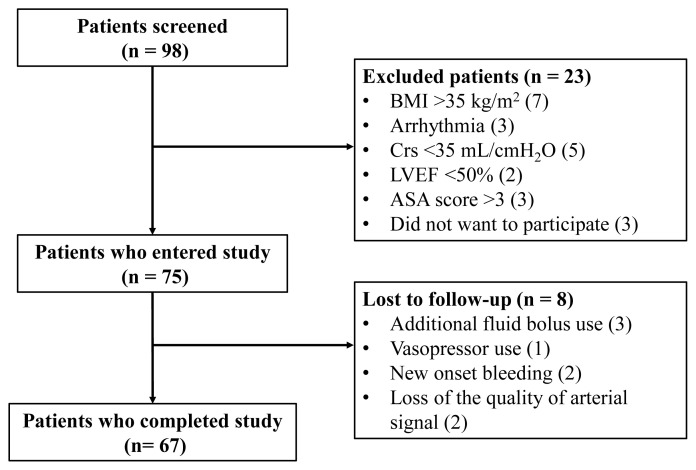
Materials and methods: The SVI, CPI, SVV, and PPV were recorded before 100 mL of isotonic saline was infused (MFC), after MFC was completed, and after an additional 400 mL of isotonic saline was infused to complete 500 mL of fluid loading (FL). Patients whose SVI increased more than 15% after the FL were defined as fluid responders.
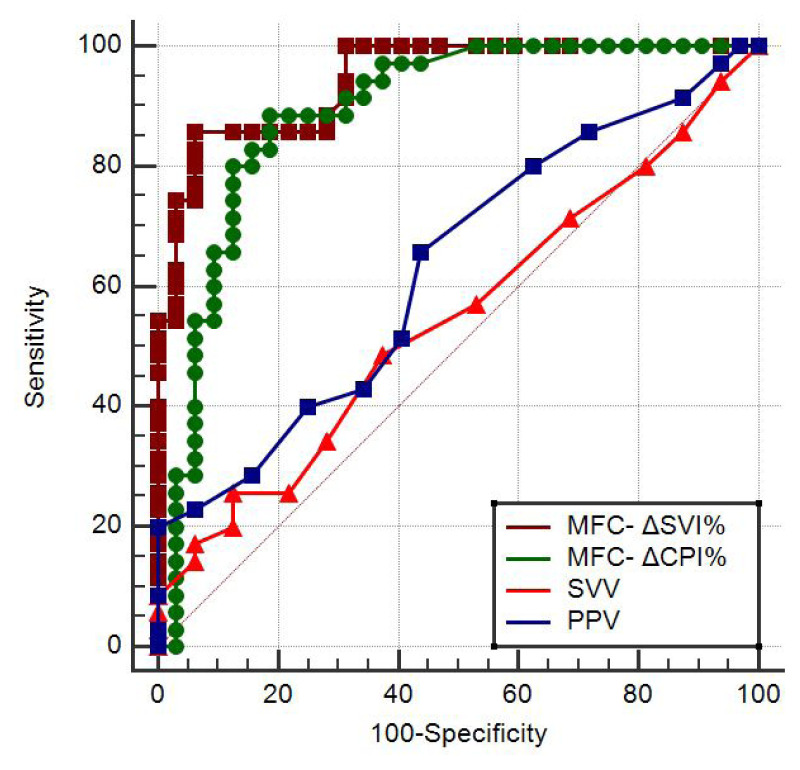
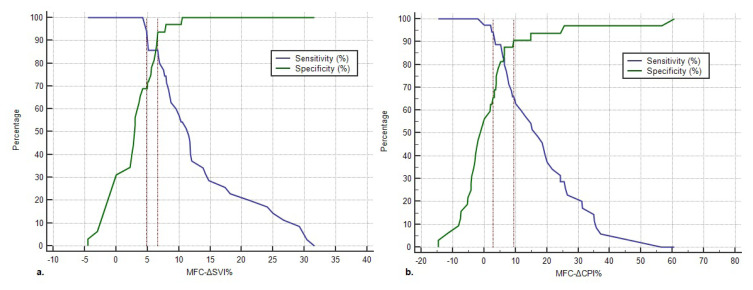
Results: Sixty-seven patients completed the study and 35 (52%) of them were responders.The areas under the receiver operating characteristics curves for the MFC-ΔSVI% and MFC-ΔCPI% (0.94; 95% CI: 0.86-0.99 and 0.89; 95% CI: 0.79-0.95, respectively) were significantly higher than those for the SVV and PPV (0.63; 95% CI: 0.50-0.75 and 0.55; 95% CI: 0.42-0.67, respectively) (p < 0.001 for all of the comparisons). The gray zone analysis revealed that the MFC-ΔSVI% values of 12 patients were in the gray zone. Of the 12, the MFC-ΔCPI% values of 7 patients were outside of the gray zone.
Conclusion: Fluid responsiveness can be predicted more accurately using the MFC-ΔSVI% and MFC-ΔCPI% than using the SVV and PPV. Additionally, concomitant use of the MFC-ΔSVI% and MFC-ΔCPI% is recommended, as this approach diminishes the number of patients in the gray zone.
Keywords: Intraoperative monitoring; fluid therapy; positive-pressure respiration; stroke volume.
© TÜBİTAK.
Conflict of interest statement
Conflict of interest: The authors declare that there are no conflicts of interest/competing interests.
Figures
Similar articles
-
Accuracy of stroke volume variation and pulse pressure variation to predict fluid responsiveness in patients with thoracic kyphosis.Ann Palliat Med. 2021 Jul;10(7):7571-7578. doi: 10.21037/apm-21-1211. Epub 2021 Jun 21. Ann Palliat Med. 2021. PMID: 34154341
-
Ability of mini-fluid challenge to predict fluid responsiveness in obese patients undergoing surgery in the prone position.Minerva Anestesiol. 2019 Sep;85(9):981-988. doi: 10.23736/S0375-9393.19.13276-2. Epub 2019 Apr 16. Minerva Anestesiol. 2019. PMID: 30994311
-
[Stroke volume and pulse pressure variation are good predictors of fluid responsiveness in sepsis patients].Acta Med Croatica. 2013 Dec;67(5):407-14. Acta Med Croatica. 2013. PMID: 24979881 Croatian.
-
Accuracy of stroke volume variation compared with pleth variability index to predict fluid responsiveness in mechanically ventilated patients undergoing major surgery.Eur J Anaesthesiol. 2010 Jun;27(6):555-61. doi: 10.1097/EJA.0b013e328335fbd1. Eur J Anaesthesiol. 2010. PMID: 20035228
-
Reliability of pulse pressure and stroke volume variation in assessing fluid responsiveness in the operating room: a metanalysis and a metaregression.Crit Care. 2023 Nov 8;27(1):431. doi: 10.1186/s13054-023-04706-0. Crit Care. 2023. PMID: 37940953 Free PMC article.
References
-
- Kumar A, Anel R, Bunnell E, Habet K, Zanotti S, et al. Pulmonary artery occlusion pressure and central venous pressure fail to predict ventricular filling volume, cardiac performance, or the response to volume infusion in normal subjects. Critical Care Medicine. 2004;32:691–699. doi: 10.1097/01.ccm.0000114996.68110.c9. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical