Serum amylase on postoperative day one is a strong predictor of pancreatic fistula after pancreaticoduodenectomy: a retrospective cohort
- PMID: 38813023
- PMCID: PMC10763807
- DOI: 10.55730/1300-0144.5693
Serum amylase on postoperative day one is a strong predictor of pancreatic fistula after pancreaticoduodenectomy: a retrospective cohort
Abstract
Background/aim: Early identification of patients at risk for developing postoperative pancreatic fistula (POPF) after pancreaticoduodenectomy (PD) may facilitate drain management. In this context, it was aimed to examine the efficiency of the serum amylase (SA) value on postoperative day (PoD) 1 in predicting the occurrence of POPF.
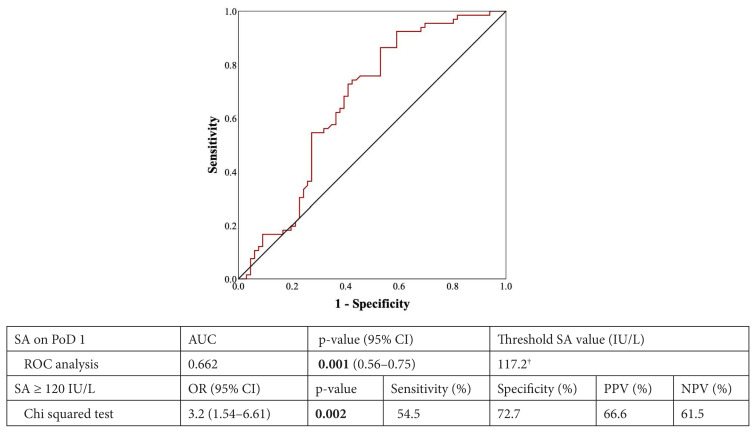
Materials and methods: A total of 132 patients who underwent PD were studied. Occurrences of POPF were classified according to the International Study Group on Pancreatic Fistula classification as a biochemical leak (BL) or clinically relevant grade b/c POPF (CR-POPF). Receiver operating characteristic analysis identified a threshold value of SA on PoD 1 associated with POPF formation.
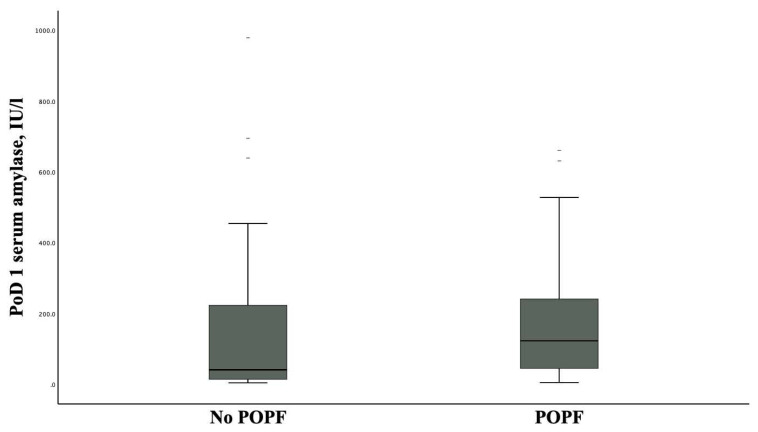
Results: Overall, 66 (50%) patients had POPF, including 51 (38.7%) with BL and 15 with CR-POPF (11.3%). The threshold value of SA associated with the development of POPF was 120 IU/L (odds ratio [OR]: 3.20; p = 0.002). In the multivariate analysis, independent POPF risk factors were SA ≥120 IU/L, soft pancreatic texture, and high-risk pathology (i.e., duodenal, biliary, ampullary, islet cell, and benign tumors); SA ≥120 IU/L outperformed soft pancreatic texture and high-risk pathology in predicting POPF, respectively (OR: 2.22; p = 0.004 vs. OR: 1.37; p = 0.012 vs. OR: 1.35; p = 0.018). In a subset analysis according to gland texture (soft vs. hard), patients with soft pancreatic texture exhibited a significantly higher incidence of POPF (63.4% vs. 34.4%) and SA ≥120 IU/L (52.1% vs. 27.9%); SA <120 IU/L had a negative predictive value of 82.5% for developing POPF in patients with hard pancreatic texture (OR: 4.28, p = 0.028).
Conclusion: A SA value ≥120 IU/L on the day after PD, which is the strongest predictor for POPF, can be used as a biomarker of the occurrence of POPF. The advantage of SA measurement is that it can contribute to identifying suitable patients for early drain removal.
Keywords: Gland palpation; gland softness; pancreas texture; whipple.
© TÜBİTAK.
Conflict of interest statement
Conflict of interest: The authors declare that there are no conflicts of interest.
Figures
Similar articles
-
Serum amylase on the night of surgery predicts clinically significant pancreatic fistula after pancreaticoduodenectomy.HPB (Oxford). 2014 Jul;16(7):610-9. doi: 10.1111/hpb.12184. Epub 2013 Nov 7. HPB (Oxford). 2014. PMID: 24246024 Free PMC article.
-
Risk scoring system and predictor for clinically relevant pancreatic fistula after pancreaticoduodenectomy.World J Gastroenterol. 2015 May 21;21(19):5926-33. doi: 10.3748/wjg.v21.i19.5926. World J Gastroenterol. 2015. PMID: 26019457 Free PMC article.
-
Predictive value of postoperative serum lipase level for postoperative pancreatic fistula after pancreaticoduodenectomy.Hepatobiliary Pancreat Dis Int. 2025 Apr;24(2):197-205. doi: 10.1016/j.hbpd.2025.01.002. Epub 2025 Jan 31. Hepatobiliary Pancreat Dis Int. 2025. PMID: 39920036
-
Drain fluid biomarkers for the diagnosis of clinically relevant postoperative pancreatic fistula: a diagnostic accuracy systematic review and meta-analysis.Int J Surg. 2023 Aug 1;109(8):2486-2499. doi: 10.1097/JS9.0000000000000482. Int J Surg. 2023. PMID: 37216227 Free PMC article.
-
Biochemical Early Detection of Postoperative Pancreatic Fistula.Visc Med. 2025 Apr 4:1-9. doi: 10.1159/000545091. Online ahead of print. Visc Med. 2025. PMID: 40330638 Free PMC article. Review.
Cited by
-
Letter to the editor: Serum amylase on postoperative day one is a strong predictor of pancreatic fistula after pancreaticoduodenectomy: a retrospective cohort.Turk J Med Sci. 2023 Dec 4;54(1):366-367. doi: 10.55730/1300-0144.5799. eCollection 2024. Turk J Med Sci. 2023. PMID: 38812626 Free PMC article. No abstract available.
-
Risk Factors For Progression From Biochemical Leak to Clinically Relevant Postoperative Pancreatic Fistula After Pancreaticoduodenectomy. The Key of the Lock: Prognostic Nutritional Index.Turk J Gastroenterol. 2024 Nov 4;36(2):100-106. doi: 10.5152/tjg.2024.24425. Turk J Gastroenterol. 2024. PMID: 39632785 Free PMC article.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical