

TARGET: A phase I/II open-label multicenter study to assess safety and efficacy of fexagratinib in patients with relapsed/refractory FGFR fusion-positive glioma
- PMID: 38813112
- PMCID: PMC11135358
- DOI: 10.1093/noajnl/vdae068
TARGET: A phase I/II open-label multicenter study to assess safety and efficacy of fexagratinib in patients with relapsed/refractory FGFR fusion-positive glioma
Abstract
Background: Oncogenic FGFR-TACC fusions are present in 3-5% of high-grade gliomas (HGGs). Fexagratinib (AZD4547) is an oral FGFR1-3 inhibitor with preclinical activity in FGFR-TACC+ gliomas. We tested its safety and efficacy in patients with recurrent FGFR-TACC + HGGs.
Patients and methods: TARGET (NCT02824133) is a phase I/II open-label multicenter study that included adult patients with FGFR-TACC + HGGs relapsing after ≥1 line of standard chemoradiation. Patients received fexagratinib 80 mg bd on a continuous schedule until disease progression or unacceptable toxicity. The primary endpoint was the 6-month progression-free survival rate (PFS6).
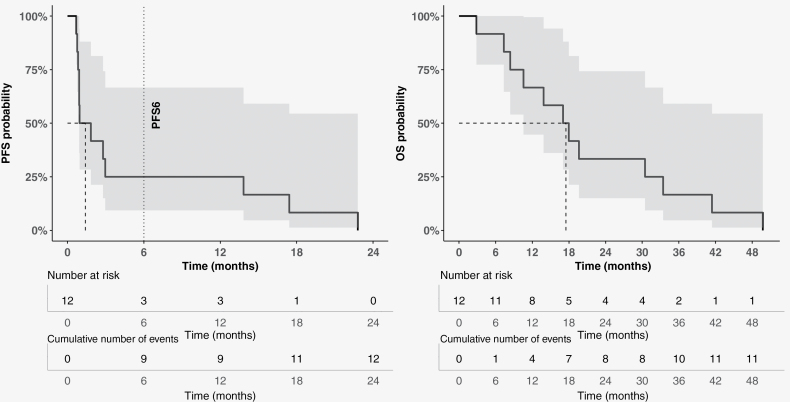
Results: Twelve patients with recurrent IDH wildtype FGFR-TACC + HGGs (all FGFR3-TACC3+) were included in the efficacy cohort (male/female ratio = 1.4, median age = 61.5 years). Most patients (67%) were included at the first relapse. The PFS6 was 25% (95% confidence interval 5-57%), with a median PFS of 1.4 months. All patients without progression at 6 months (n = 3) were treated at first recurrence (versus 56% of those in progression) and remained progression-free for 14-23 months. The best response was RANO partial response in 1 patient (8%), stable disease in 5 (42%), and progressive disease in 6 (50%). Median survival was 17.5 months from inclusion. Grade 3 toxicities included lymphopenia, hyperglycaemia, stomatitis, nail changes, and alanine aminotransferase increase (n = 1 each). No grade 4-5 toxicities were seen. A 32-gene signature was associated with the benefit of FGFR inhibition in FGFR3-TACC3 + HGGs.
Conclusions: Fexagratinib exhibited acceptable toxicity but limited efficacy in recurrent FGFR3-TACC3 + HGGs. Patients treated at first recurrence appeared more likely to benefit, yet additional evidence is required.
Keywords: FGFR inhibitor; FGFR3–TACC3; clinical trial; fexagratinib; glioblastoma; glioma.
© The Author(s) 2024. Published by Oxford University Press, the Society for Neuro-Oncology and the European Association of Neuro-Oncology.
Conflict of interest statement
A.P. and M.S. declare having received travel support from Astra Zeneca. The other authors have declared no conflict of interest relevant to this paper.
Figures


References
-
- Sanson M, Marie Y, Paris S, et al.. Isocitrate dehydrogenase 1 codon 132 mutation is an important prognostic biomarker in gliomas. J Clin Oncol. 2009;27(25):4150–4154. - PubMed
-
- Stupp R, Mason WP, van den Bent MJ, et al.; European Organisation for Research and Treatment of Cancer Brain Tumor and Radiotherapy Groups. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. 2005;352(10):987–996. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous