

Intraperitoneal Liposarcoma: A Case Report and Literature Review of a Rare Entity
- PMID: 38813304
- PMCID: PMC11134115
- DOI: 10.7759/cureus.59244
Intraperitoneal Liposarcoma: A Case Report and Literature Review of a Rare Entity
Abstract
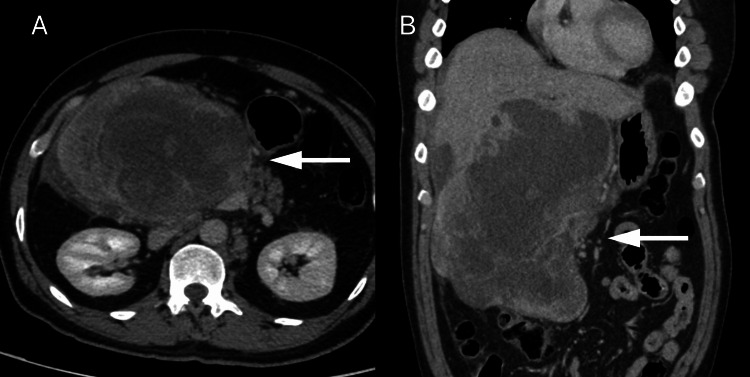
Liposarcoma is a rare soft-tissue neoplasm originating from adipocytes. The exact cause of liposarcoma is unknown and symptoms vary depending on the tumor's location. A 49-year-old man presented to the emergency room complaining of epigastric pain radiating to the back and right upper quadrant. Cross-sectional imaging revealed a large upper abdominal mass that was thought to be a gastrointestinal stromal tumor (GIST) arising from the duodenum at first. The patient underwent en-bloc resection of the mass and was planned for adjuvant chemotherapy. Subsequently, multiple tissue samples were examined, leading to the final diagnosis of de-differentiated liposarcoma. The patient eventually developed multiple recurrences and was subjected to re-resection surgeries and three different chemotherapy regimens. Given the rarity of the disease, no standardized therapy plan is available, highlighting the need for more case reports/series and trials to broaden our understanding of this disease.
Keywords: dedifferentiated liposarcoma; intra-peritoneal; liposarcoma; mdm2; recurrent sarcoma.
Copyright © 2024, AlBathi et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures




Similar articles
-
Intraperitoneal dedifferentiated liposarcoma showing MDM2 amplification: case report.World J Surg Oncol. 2013 Nov 26;11:305. doi: 10.1186/1477-7819-11-305. World J Surg Oncol. 2013. PMID: 24279301 Free PMC article.
-
Surgery of intraabdominal giant dedifferentiated liposarcoma of ascending colon mesentery: A rare case report.Int J Surg Case Rep. 2022 Sep;98:107482. doi: 10.1016/j.ijscr.2022.107482. Epub 2022 Aug 10. Int J Surg Case Rep. 2022. PMID: 35973321 Free PMC article.
-
Dedifferentiated liposarcoma with a rare presentation of disseminated intraperitoneal sarcomatosis: A case report.Int J Surg Case Rep. 2019;60:331-335. doi: 10.1016/j.ijscr.2019.06.051. Epub 2019 Jun 26. Int J Surg Case Rep. 2019. PMID: 31280066 Free PMC article.
-
A challenging diagnosis of mesenchymal neoplasm of the colon: colonic dedifferentiated liposarcoma with lymph node metastases-a case report and review of the literature.Int J Colorectal Dis. 2019 Oct;34(10):1809-1814. doi: 10.1007/s00384-019-03394-z. Epub 2019 Sep 9. Int J Colorectal Dis. 2019. PMID: 31501928 Review.
-
Paratesticular Dedifferentiated Liposarcoma with Rhabdomyoblastic Differentiation: A Case Report and Review of the Literature.Prague Med Rep. 2023;124(4):449-455. doi: 10.14712/23362936.2023.35. Prague Med Rep. 2023. PMID: 38069650 Review.
References
-
- Liposarcomas: diagnostic pitfalls and new insights. Dei Tos AP. Histopathology. 2014;64:38–52. - PubMed
-
- Dedifferentiated liposarcoma: a clinicopathological analysis of 155 cases with a proposal for an expanded definition of dedifferentiation. Henricks WH, Chu YC, Goldblum JR, Weiss SW. Am J Surg Pathol. 1997;21:271–281. - PubMed
-
- Omental liposarcoma presenting as chronic constipation. Hightower JL Jr, Dire DJ. Pediatr Emerg Care. 2014;30:483–484. - PubMed
-
- Retroperitoneal or mesenteric primary liposarcoma: clinical and prognostic evaluations on five cases. RO L, SU LP, BE L, PE P, CO E, MO G. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5902147/ G Chir. 2018;39:57–62. - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials