

The impact of right bundle branch block and SIQIII-type patterns in determining risk levels in acute pulmonary embolism
- PMID: 38813350
- PMCID: PMC11134142
- DOI: 10.12688/f1000research.131758.1
The impact of right bundle branch block and SIQIII-type patterns in determining risk levels in acute pulmonary embolism
Abstract
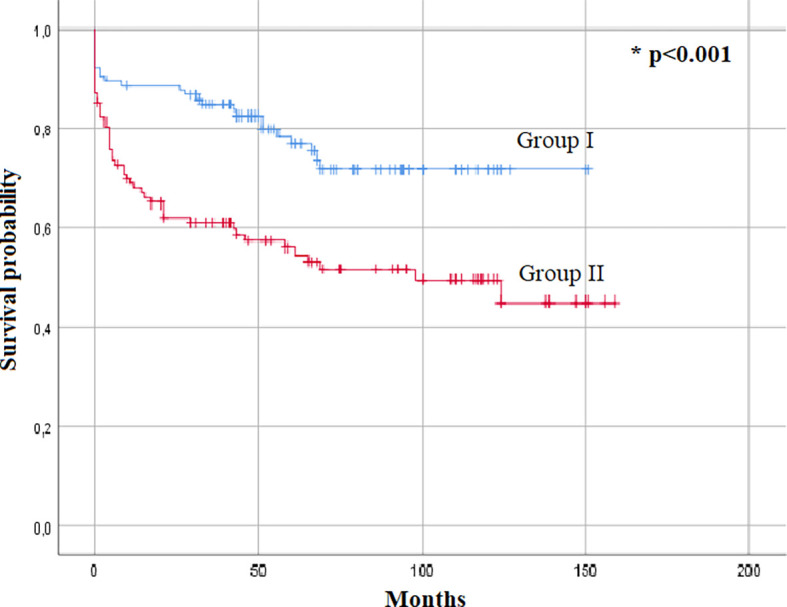
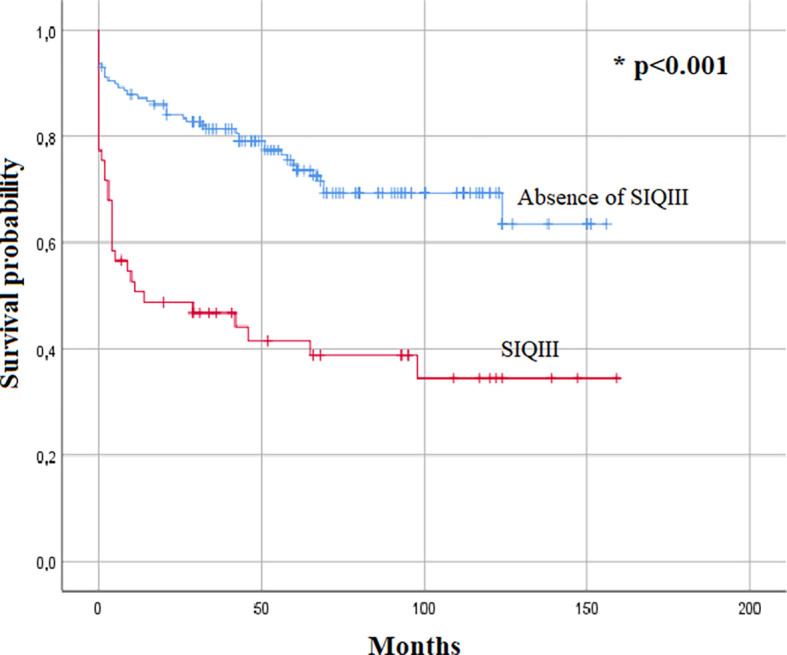
Background: Electrocardiography (ECG) findings in acute pulmonary embolism (PE) are known to be related to various right ventricular (RV) alterations. These abnormalities are not included in risk stratification algorithms despite emerging evidence of their association with patient outcomes. We aimed to analyze the impact of right bundle branch block (RBBB) and/or SIQIII patterns as indicators for determining the level of risk in patients with PE. Methods: We performed a retrospective cohort study including all patients with confirmed acute PE hospitalized from January 2008 to December 2019 in two tertiary care cardiology departments. The first ECG taken at admission was selected and the analysis focused on the presence of a complete or an incomplete RBBB and SIQIII-type patterns. Results: A total of 255 patients were divided into two groups: Group I (47.8%, n=122) included patients with PE without RBBB nor SIQIII patterns, and Group II (52.2%, n=133) included patients with RBBB and/or SIQIII patterns. Patients in group II presented significantly more frequently with acute right heart symptoms (45.1% vs. 18%, p<0.001) and cardiogenic shock at admission (31.6 vs. 4.1%, p<0.001). Echocardiographic parameters indicating right heart injury also occurred more significantly in group II patients (p<0.001). By univariate analysis, patients in group II were found to be significantly associated with in-hospital mortality (22.6 vs. 6.1%, p=0.002) and major cardiovascular events (MACEs) during hospitalization (43.3 vs. 13.7%, p<0.001). Multivariate logistic regression analysis identified five independent factors predictive of MACEs: SIQIII and/or RBBB, renal failure, positive troponin levels, RV dysfunction and right heart failure symptoms during initial presentation. Kaplan-Meier survival analysis identified the inclusion in Group II and the presence of SIQIII pattern as predictors of overall mortality (p<0.001). Conclusions: Our study suggests an important and independent prognostic value of RBBB and SIQIII patterns and their usefulness in determining the outcome of PE patients.
Keywords: Electrocardiogram; Mortality; Prognosis; Pulmonary embolism.
Copyright: © 2023 Hassine M et al.
Conflict of interest statement
No competing interests were disclosed.
Figures
Similar articles
-
Right bundle branch block and SIQIII-type patterns for risk stratification in acute pulmonary embolism.J Electrocardiol. 2016 Jul-Aug;49(4):512-8. doi: 10.1016/j.jelectrocard.2016.03.020. Epub 2016 Mar 29. J Electrocardiol. 2016. PMID: 27083328
-
Primary angioplasty in acute myocardial infarction with right bundle branch block: should new onset right bundle branch block be added to future guidelines as an indication for reperfusion therapy?Eur Heart J. 2012 Jan;33(1):86-95. doi: 10.1093/eurheartj/ehr291. Epub 2011 Sep 1. Eur Heart J. 2012. PMID: 21890488 Free PMC article.
-
Electrocardiography changes and their significance during treatment of patients with intermediate-high and high-risk pulmonary embolism.Eur Heart J Acute Cardiovasc Care. 2020 Jun;9(4):271-278. doi: 10.1177/2048872618823441. Epub 2019 Jan 11. Eur Heart J Acute Cardiovasc Care. 2020. PMID: 30632764
-
Association of different electrocardiographic patterns with shock index, right ventricle systolic pressure and diameter, and embolic burden score in pulmonary embolism.Vojnosanit Pregl. 2016 Oct;73(10):921-6. doi: 10.2298/VSP150512011K. Vojnosanit Pregl. 2016. PMID: 29327898
-
The value of electrocardiographic abnormalities in the prognosis of pulmonary embolism: a consensus paper.Ann Noninvasive Electrocardiol. 2015 May;20(3):207-23. doi: 10.1111/anec.12278. Ann Noninvasive Electrocardiol. 2015. PMID: 25994548 Free PMC article. Review.
References
-
- Stein PD, Dalen JE, Mclntyre KM, et al. : The Electrocardiogram in Acute Pulmonary Embolism. - PubMed
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical