

Diabetic and hypertensive disorders following early pregnancy loss: a systematic review and meta-analysis
- PMID: 38813443
- PMCID: PMC11133813
- DOI: 10.1016/j.eclinm.2024.102560
Diabetic and hypertensive disorders following early pregnancy loss: a systematic review and meta-analysis
Abstract
Background: Spontaneous and induced abortions are common outcomes of pregnancy. There is inconsistent evidence of an association between early pregnancy loss and subsequent diabetic and hypertensive disorders in women. This systematic review and meta-analysis evaluated evidence on the risk of the subsequent development of pregnancy and non-pregnancy related diabetic and hypertensive disorders in women who experienced an early pregnancy loss.
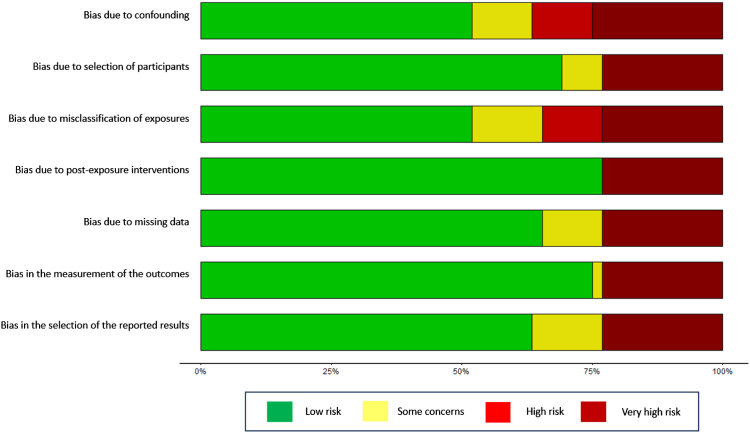
Methods: Systematic searches were conducted in seven electronic databases (CINAHL Plus, Ovid/EMBASE, Ovid/MEDLINE, ProQuest, PubMed, Scopus, and Web of Science) from inception to 22nd December 2023. Studies were included if they reported an exposure of spontaneous abortion (SAB), induced abortion (IA) or recurrent pregnancy loss (RPL) with an outcome of gestational diabetes mellitus, pre-eclampsia, gestational hypertension, and non-pregnancy related diabetic and hypertensive disorders. Risk of bias was assessed using Risk of Bias Instrument for Non-Randomized Studies of Exposures (ROBINS-E). Random effects meta-analysis was used to pool odds of developing diabetic and hypertensive disorders following an early pregnancy loss. This study is registered with PROSPERO (CRD42022327689).
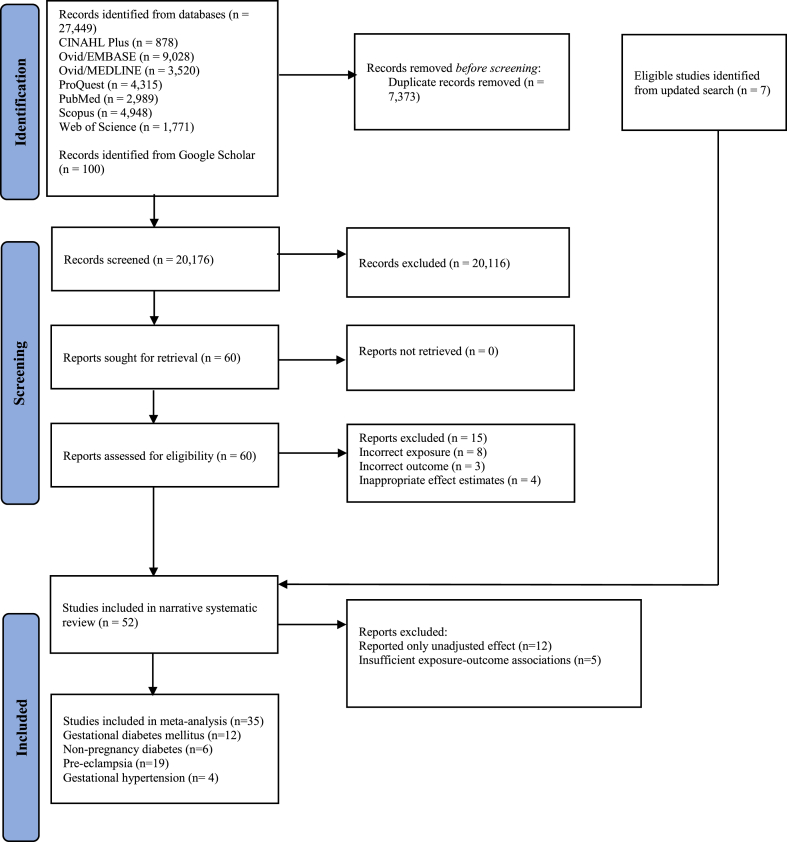
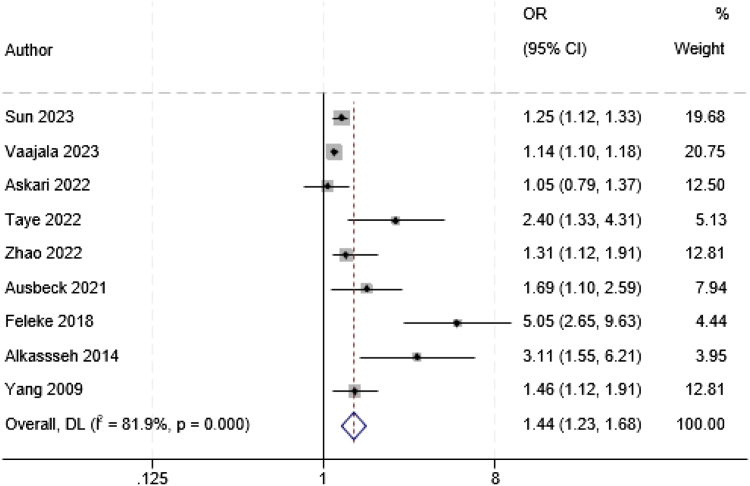
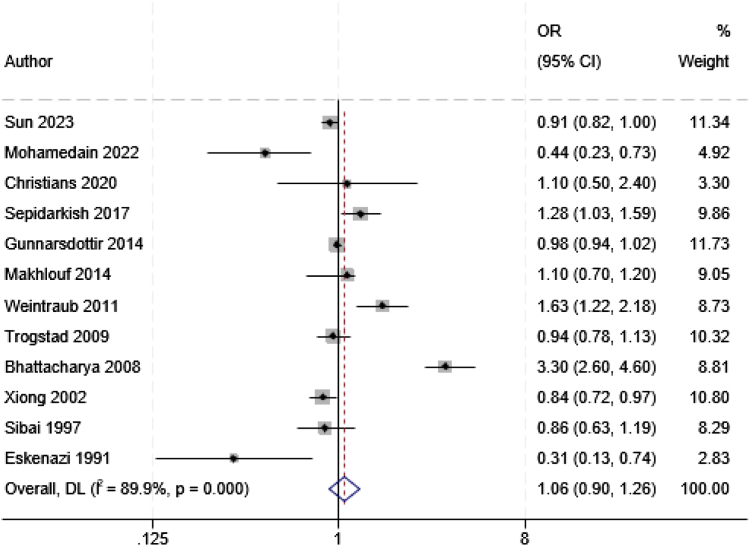
Findings: Of 20,176 records, 60 unique articles were identified for full-text review and 52 met the inclusion criteria, representing a total population of 4,132,895 women from 22 countries. Thirty-five studies were suitable for meta-analysis, resulting in a pooled odds ratio (OR) of 1.44 (95% confidence interval (CI) 1.23-1.68) for gestational diabetes mellitus following a prior SAB and a pooled OR of 1.06 (95% CI 0.90-1.26) for pre-eclampsia following a prior SAB. RPL increased the odds of developing pre-eclampsia (OR 1.37 95% CI 1.05-1.79). There was no association between IA and diabetic and hypertensive disorders.
Interpretation: A prior SAB was associated with increased odds of gestational diabetes mellitus, but not pre-eclampsia. However, women who experienced RPL had an increased risk of subsequent pre-eclampsia. Future research is required to establish evidence for an association between early pregnancy loss with non-pregnancy related diabetic and hypertensive disorders.
Funding: National Health and Medical Research Council.
Keywords: Abortion; Diabetes; Hypertension; Miscarriage; Pre-eclampsia.
© 2024 The Authors.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Diabetic and Hypertensive Disorders Following Miscarriage: A Protocol for Systematic Review and Meta-Analysis.Int J Environ Res Public Health. 2022 Jul 7;19(14):8324. doi: 10.3390/ijerph19148324. Int J Environ Res Public Health. 2022. PMID: 35886173 Free PMC article.
-
Calcium supplementation commencing before or early in pregnancy, for preventing hypertensive disorders of pregnancy.Cochrane Database Syst Rev. 2019 Sep 16;9(9):CD011192. doi: 10.1002/14651858.CD011192.pub3. Cochrane Database Syst Rev. 2019. PMID: 31523806 Free PMC article.
-
Association between maternal thyroid function and risk of gestational hypertension and pre-eclampsia: a systematic review and individual-participant data meta-analysis.Lancet Diabetes Endocrinol. 2022 Apr;10(4):243-252. doi: 10.1016/S2213-8587(22)00007-9. Epub 2022 Mar 4. Lancet Diabetes Endocrinol. 2022. PMID: 35255260 Free PMC article.
-
Association between hypertensive disorders of pregnancy and the risk of asthma, eczema and allergies in offspring: A systematic review and meta-analysis.Clin Exp Allergy. 2021 Jan;51(1):29-38. doi: 10.1111/cea.13754. Epub 2020 Oct 23. Clin Exp Allergy. 2021. PMID: 33037716
-
Metformin for prevention of hypertensive disorders of pregnancy in women with gestational diabetes or obesity: systematic review and meta-analysis of randomized trials.Ultrasound Obstet Gynecol. 2018 Dec;52(6):706-714. doi: 10.1002/uog.19084. Epub 2018 Nov 1. Ultrasound Obstet Gynecol. 2018. PMID: 29749110
Cited by
-
Exploring user profiles and preferences for mobile apps promoting active lifestyles during pregnancy and postpartum: cross-sectional study.BMC Pregnancy Childbirth. 2025 May 10;25(1):558. doi: 10.1186/s12884-025-07635-8. BMC Pregnancy Childbirth. 2025. PMID: 40348982 Free PMC article.
-
Association of spontaneous abortion and lifestyle with diabetes mellitus in women: a cross-sectional study in UK Biobank.BMC Pregnancy Childbirth. 2025 Mar 27;25(1):362. doi: 10.1186/s12884-025-07461-y. BMC Pregnancy Childbirth. 2025. PMID: 40148801 Free PMC article.
-
Women's physical health around live births and pregnancy losses: a longitudinal study.Eur J Public Health. 2025 Apr 1;35(2):335-341. doi: 10.1093/eurpub/ckaf013. Eur J Public Health. 2025. PMID: 39933033 Free PMC article.
-
"Unraveling the Clot-Miscarriage Nexus: Mechanisms, Management, and Future Directions in Thrombosis-Related Recurrent Pregnancy Loss".Clin Appl Thromb Hemost. 2025 Jan-Dec;31:10760296251339421. doi: 10.1177/10760296251339421. Epub 2025 Apr 29. Clin Appl Thromb Hemost. 2025. PMID: 40302365 Free PMC article. Review.
References
-
- Christou A., Dibley M.J., Raynes-Greenow C. Beyond counting stillbirths to understanding their determinants in low- and middle-income countries: a systematic assessment of stillbirth data availability in household surveys. Trop Med Int Health. 2017;22(3):294–311. doi: 10.1111/tmi.12828. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
