

Gut microbiome correlates of recurrent urinary tract infection: a longitudinal, multi-center study
- PMID: 38813445
- PMCID: PMC11133793
- DOI: 10.1016/j.eclinm.2024.102490
Gut microbiome correlates of recurrent urinary tract infection: a longitudinal, multi-center study
Abstract
Background: Urinary tract infections (UTI) affect approximately 250 million people annually worldwide. Patients often experience a cycle of antimicrobial treatment and recurrent UTI (rUTI) that is thought to be facilitated by a gut reservoir of uropathogenic Escherichia coli (UPEC).
Methods: 125 patients with UTI caused by an antibiotic-resistant organism (ARO) were enrolled from July 2016 to May 2019 in a longitudinal, multi-center cohort study. Multivariate statistical models were used to assess the relationship between uropathogen colonization and recurrent UTI (rUTI), controlling for clinical characteristics. 644 stool samples and 895 UPEC isolates were interrogated for taxonomic composition, antimicrobial resistance genes, and phenotypic resistance. Cohort UTI gut microbiome profiles were compared against published healthy and UTI reference microbiomes, as well as assessed within-cohort for timepoint- and recurrence-specific differences.
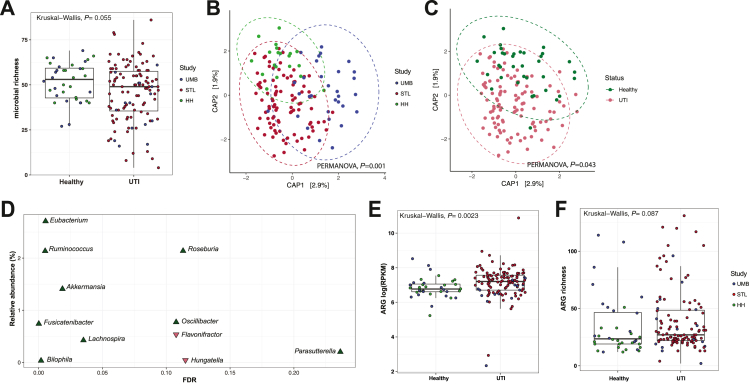
Findings: Risk of rUTI was not independently associated with clinical characteristics. The UTI gut microbiome was distinct from healthy reference microbiomes in both taxonomic composition and antimicrobial resistance gene (ARG) burden, with 11 differentially abundant taxa at the genus level. rUTI and non-rUTI gut microbiomes in the cohort did not generally differ, but gut microbiomes from urinary tract colonized patients were elevated in E. coli abundance 7-14 days post-antimicrobial treatment. Corresponding UPEC gut isolates from urinary tract colonizing lineages showed elevated phenotypic resistance against 11 of 23 tested drugs compared to non-colonizing lineages.
Interpretation: The gut microbiome is implicated in UPEC urinary tract colonization during rUTI, serving as an ARG-enriched reservoir for UPEC. UPEC can asymptomatically colonize the gut and urinary tract, and post-antimicrobial blooms of gut E. coli among urinary tract colonized patients suggest that cross-habitat migration of UPEC is an important mechanism of rUTI. Thus, treatment duration and UPEC populations in both the urinary and gastrointestinal tract should be considered in treating rUTI and developing novel therapeutics.
Funding: This work was supported in part by awards from the U.S. Centers for Disease Control and Prevention Epicenter Prevention Program (grant U54CK000482; principal investigator, V.J.F.); to J.H.K. from the Longer Life Foundation (an RGA/Washington University partnership), the National Center for Advancing Translational Sciences (grants KL2TR002346 and UL1TR002345), and the National Institute of Allergy and Infectious Diseases (NIAID) (grant K23A1137321) of the National Institutes of Health (NIH); and to G.D. from NIAID (grant R01AI123394) and the Eunice Kennedy Shriver National Institute of Child Health and Human Development (grant R01HD092414) of NIH. R.T.'s research was funded by the Deutsche Forschungsgemeinschaft (DFG; German Research Foundation; grant 402733540). REDCap is Supported by Clinical and Translational Science Award (CTSA) Grant UL1 TR002345 and Siteman Comprehensive Cancer Center and NCI Cancer Center Support Grant P30 CA091842. The content is solely the responsibility of the authors and does not necessarily represent the official views of the funding agencies.
Keywords: Antimicrobial resistance; Escherichia coli; Gut microbiome; Recurrent urinary tract infection.
© 2024 The Authors.
Conflict of interest statement
E.R.D. reports grants from Theriva Biologics, trial enrollment support and consulting fees from Ferring, and consulting fees from Seres. V.F. reports grants from The Foundation for Barnes-Jewish Hospital, grants from Doris Duke Charitable Foundation, grants from NIH/NCATS (project numbers KL2TR002346, UL1TR002345), and royalties/licenses from Elsevier (Goldman-Cecil Medicine, 2-Volume Set, 27e). She has served various roles at the Infectious Diseases Society of America (Board of Directors 2017–2020, IDSA Leadership Institute 2018–2022, Editor-in-Chief Search Committee Chair of the Open Forum Infectious Disease Journal 2022). Her spouse is a consultant and former Senior Vice President/Chief Medical Officer at Cigna/Express-Scripts. M.A.O. reports consulting fees from Pfizer. C.A.B. reports paid roles as editor at the Journal of Clinical Microbiology, and unpaid roles with the Clinical and Laboratory Standards Institute. She has served as Chief Clinical Officer at Pattern Bioscience since 2022 and holds shares. All other authors declare no conflict of interests.
Figures


References
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
