

Clinical manifestations and long-term symptoms associated with SARS-CoV-2 omicron infection in children aged 0-17 years in Beijing: a single-center study
- PMID: 38813546
- PMCID: PMC11133534
- DOI: 10.3389/fped.2024.1332020
Clinical manifestations and long-term symptoms associated with SARS-CoV-2 omicron infection in children aged 0-17 years in Beijing: a single-center study
Abstract
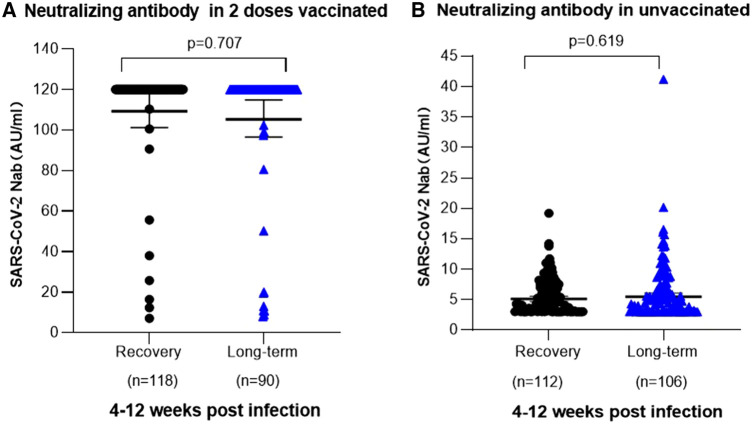
Objective: The study aims to analyze the clinical characteristics of acute phase of SARS-CoV-2 infection in children aged 0-17 years with the Omicron variant, and summarize the persistent symptoms or new-onset clinical manifestations from 4 to 12 weeks after acute COVID. Explore the association between the vaccination status and SARS-CoV-2 neutralizing antibody levels post infection among preschool-aged children. The comprehensive study systematically describes the clinical characteristics of children infected with SARS-CoV-2, providing a foundation for diagnosis and evaluating long-term COVID in pediatric populations.
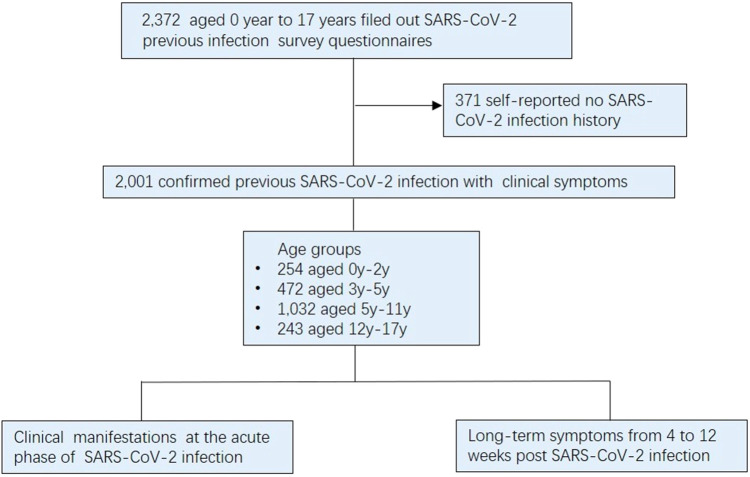
Methods: The study enrolled children who were referred to the Children's Hospital, Capital Institute of Pediatrics, (Beijing, China) from January 10, 2023 to March 31, 2023. Participants were classified as infant and toddlers, preschool, school-age, and adolescent groups. Children or their legal guardians completed survey questionnaires to provide information of previous SARS-CoV-2 infection history, as well as clinical presentation during the acute phase and long-term symptoms from 4 to 12 weeks following infection. Furthermore, serum samples were collected from children with confirmed history of SARS-CoV-2 infection for serological testing of neutralizing antibodies.
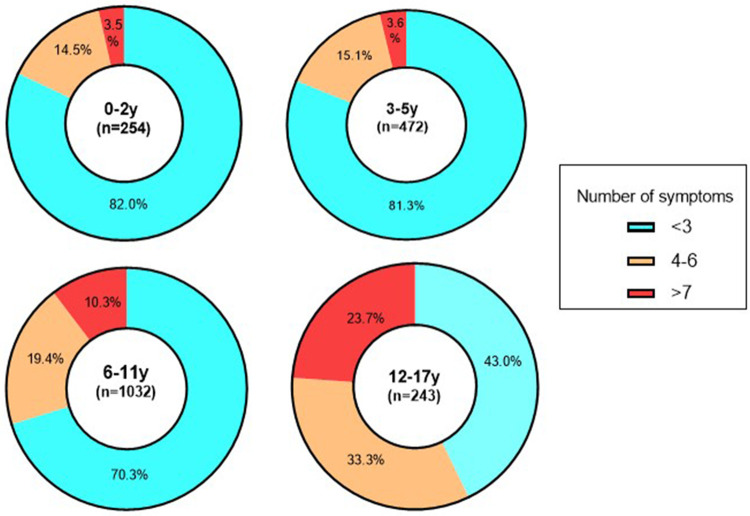
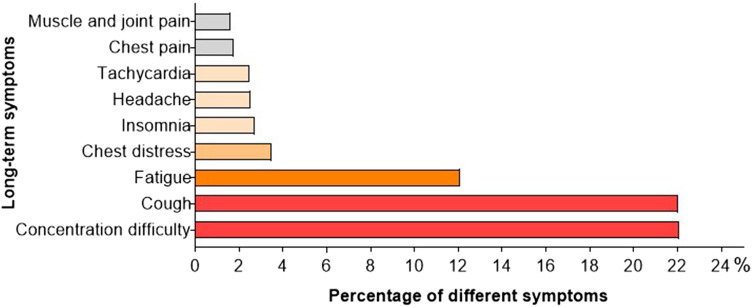
Results: The study recruited a total of 2,001 children aged 0-17 years who had previously tested positive for SARS-CoV-2 through nucleic acid or antigen testing. Fever emerged as the predominant clinical manifestation in 1,902 (95.1%) individuals with body temperature ranging from 37.3 to 40.0°C. Respiratory symptoms were identified as secondary clinical manifestations, with cough being the most common symptom in 777 (38.8%) children, followed by sore throat (22.1%), nasal congestion (17.8%), and runnning nose (17.2%). Fatigue (21.6%), headache (19.8%) and muscle-joint pain (13.5%) were frequently reported systemic symptoms in children. The proportion of children with symptoms of SARS-CoV-2 infection varied across age groups. 1,100 (55.0%) children experienced persistent symptoms from 4 to 12 weeks post the acute phase of infection. Trouble concentrating (22.1%), cough (22.1%), and fatigue (12.1%) were frequently reported across age groups in the extended period. A limited number of children exhibited cardiovascular symptoms with chest tightness, tachycardia, and chest pain reported by 3.5%, 2.5%, and 1.8% of children, respectively. Among 472 children aged 3-5 years, 208 children had received two doses of SARS-CoV-2 vaccine at least 6 months prior to infection, and no association was found between the incidence of long-term COVID and pre-infection vaccination statuses among the 3-5 years age groups (χ2 = 1.136, P = 0.286).
Conclusions: In children aged 0-17 years infected with SARS-CoV-2 Omicron variant, fever was the primary clinical manifestation in the acute phase, followed by respiratory symptoms, systemic non-specific and digestive presentations. In particular, respiratory and digestive system symptoms were more frequent in children aged above 6 years. Regarding the long-term symptoms from 4 to 12 weeks post-infection, the most common presentations were concentrating difficulty, cough, and fatigue. The incidence of persistent symptoms of SARS-CoV-2 did not exhibit a significant correlation with vaccination status, which was attributed to the waning efficacy of the vaccine-induced humoral immune response after 6 months.
Keywords: SARS-CoV-2 infection; children; long-term COVID; symptoms; vaccination.
© 2024 Li, Li, Cao, Wang, Chen, Niu, Dang, Dai, Wang, Ge, Liu, Song, Xu and Ma.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Pediatric population (aged 3-11 years) received primary inactivated SARS-CoV-2 vaccination prior to infection exhibiting robust humoral immune response following infected with Omicron variant: a study conducted in Beijing.Front Immunol. 2023 Sep 27;14:1269665. doi: 10.3389/fimmu.2023.1269665. eCollection 2023. Front Immunol. 2023. PMID: 37828994 Free PMC article.
-
[Clinical characteristics of COVID-19 Omicron variant infection in children with allergic diseases].Zhonghua Yu Fang Yi Xue Za Zhi. 2023 Sep 6;57(9):1373-1379. doi: 10.3760/cma.j.cn112150-20230419-00307. Zhonghua Yu Fang Yi Xue Za Zhi. 2023. PMID: 37743297 Chinese.
-
[Short-term persistent symptoms in preschool children with mild/common coronavirus disease 2019 caused by Omicron variant infection after discharge: a follow-up study].Zhongguo Dang Dai Er Ke Za Zhi. 2022 Dec 15;24(12):1289-1294. doi: 10.7499/j.issn.1008-8830.2206034. Zhongguo Dang Dai Er Ke Za Zhi. 2022. PMID: 36544405 Free PMC article. Chinese.
-
Italian intersociety consensus on management of long covid in children.Ital J Pediatr. 2022 Mar 9;48(1):42. doi: 10.1186/s13052-022-01233-6. Ital J Pediatr. 2022. PMID: 35264214 Free PMC article. Review.
-
Viral and antibody dynamics of acute infection with SARS-CoV-2 omicron variant (B.1.1.529): a prospective cohort study from Shenzhen, China.Lancet Microbe. 2023 Aug;4(8):e632-e641. doi: 10.1016/S2666-5247(23)00139-8. Epub 2023 Jul 14. Lancet Microbe. 2023. PMID: 37459867 Review.
References
-
- Cloete J, Kruger A, Masha M, du Plessis NM, Mawela D, Tshukudu M, et al. Paediatric hospitalisations due to COVID-19 during the first SARS-CoV-2 omicron (B.1.1.529) variant wave in South Africa: a multicentre observational study. Lancet Child Adolesc Health. (2022) 6(5):294–302. 10.1016/S2352-4642(22)00027-X - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous