

[Treatment of proximal humeral fractures in childhood and adolescence : Consensus report of the pediatric traumatology section of the German Society for Trauma Surgery]
- PMID: 38814464
- PMCID: PMC11219542
- DOI: 10.1007/s00113-024-01440-2
[Treatment of proximal humeral fractures in childhood and adolescence : Consensus report of the pediatric traumatology section of the German Society for Trauma Surgery]
Abstract
Background: Proximal humeral fractures are a relatively common injury in childhood and adolescence, accounting for 0.45-2% of all fractures [2, 18]. Treatment is usually conservative but is still the subject of a scientific debate [9, 12]. In addition to the S1-LL, there are different recommendations for the diagnostics and treatment of these fractures in the literature.
Methodology: As part of the 10th scientific meeting of the SKT of the DGU, the existing recommendations and the relevant or current literature were critically discussed by a panel of experts and a consensus was formulated. An algorithm for the diagnostics, therapy and treatment was integrated into this.
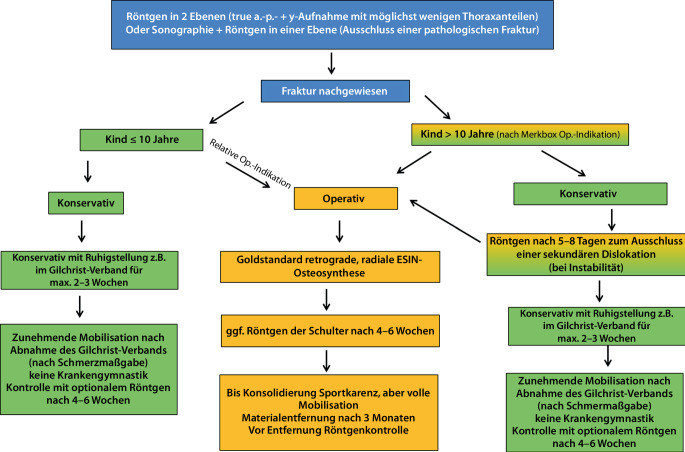
Results: The measurement of axial deviation and tilt is not interobserver and intraobserver reliable [3]. The age limit for when complete correction is possible was set at an age of 10 years, as the correction potential changes around this age. For diagnostic purposes, well-centered X‑ray images in 2 planes (true AP and Y‑images without thoracic parts) is defined as the standard. At the age of less than 10 years, any malposition can be treated conservatively with Gilchrist bandaging for 2-3 weeks. Surgery can only be indicated in individual cases, e.g., in the event of severe pain or the need for rapid weight bearing. An ad latus displacement of more than half the shaft width should not be tolerated over the age of 10 years. Due to the variance in the measurement results, it is not possible to recommend surgical treatment depending on the extent of the ad axim dislocation. As a guideline, the greater the dislocation and the closer the child is to growth joint closure, the more likely surgical treatment is indicated. The development should be taken into account. The gold standard is retrograde, radial and unilateral ESIN osteosynthesis using two intramedullary nails. Osteosynthesis does not require immobilization. A follow-up X‑ray is planned for unstable fractures without osteosynthesis after 1 week, otherwise optional for documentation of consolidation after 4-6 weeks, e.g., if sports clearance is to be granted and before metal removal (12 weeks).
Conclusion: Recommendations for surgical indications based on the extent of tilt are not reproducible and seem difficult in view of the current literature [3, 9, 12]. A pragmatic approach is recommended. The prognosis of the fracture appears to be so good, taking the algorithm into account, that restitutio ad integrum can be expected in most cases.
Zusammenfassung: HINTERGRUND: Die proximale Humerusfraktur ist mit 0,45–2 % aller Frakturen eine relativ häufige Verletzung im Kindes- und im Jugendalter [2, 18]. Die Behandlung ist meistens konservativ, aber immer noch Gegenstand der wissenschaftlichen Diskussion [9, 12]. Neben der S1-LL gibt es unterschiedliche Empfehlungen zu Diagnostik und Behandlung dieser Fraktur in der Literatur.
Methodik: Im Rahmen des 10. Wissenschaftstreffens der SKT in der DGU wurden die vorhandenen Empfehlungen und die relevante bzw. aktuelle Literatur kritisch von einem Expertengremium diskutiert und ein Konsens formuliert. In diesen wurde ein Algorithmus zu Diagnostik, Therapie und Behandlung integriert.
Ergebnisse: Die Messung der Achsabweichung und Abkippung ist nicht „interobserver“ und „intraobserver reliable“ [3]. Die Altersgrenze, bis zu der eine vollständige Korrektur möglich ist, wurde auf 10 Jahre festgelegt, da sich ca. um dieses Alter das Korrekturpotenzial ändert. Zur Diagnostik wird die gut zentrierte Röntgenaufnahme in 2 Ebenen (true a.-p.- und Y‑Aufnahme ohne Thoraxanteile) als Standard festgelegt. Im Alter unter 10 Jahren kann jegliche Fehlstellung konservativ mittels Gilchrist-Verband für 2 bis 3 Wochen behandelt werden. Nur in Einzelfällen kann eine Operation z. B. bei starken Schmerzen oder notwendiger rascher Belastbarkeit indiziert sein. Über 10 Jahren sollte ein Ad-latus-Versatz über halbe Schaftbreite nicht toleriert werden. Aufgrund der Varianz der Messergebnisse kann eine Empfehlung zur operativen Versorgung in Abhängigkeit vom Ausmaß der Ad-axim-Dislokation nicht benannt werden. Orientierend gilt: Je größer die Dislokation und je näher das Kind am Fugenschluss ist, desto eher ist die operative Therapie indiziert. Die Entwicklung ist hier einzubeziehen. Den Goldstandard stellt die retrograde, radiale und unilaterale ESIN-Osteosynthese mittels 2 intramedullären Nägeln dar. Die Osteosynthese erfordert keine Ruhigstellung. Ein Verlaufsröntgen ist bei instabilen Frakturen ohne Osteosynthese nach einer Woche, sonst optional zur Dokumentation der Konsolidierung nach 4 (bis 6) Wochen, wenn z. B. die Sportfreigabe erteilt werden soll, sowie vor der Metallentfernung (12 Wochen) vorgesehen.
Schlussfolgerung: Empfehlungen zur Operationsindikation auf der Grundlage des Ausmaßes der Abkippung sind nicht reproduzierbar und erscheinen in Anbetracht der aktuellen Literatur schwierig [3, 9, 12]. Sinnvoller ist ein pragmatisches Vorgehen. Die Prognose der Fraktur erscheint unter Beachtung des erstellten Algorithmus so gut zu sein, dass in den meisten Fällen die Restitutio ad integrum erwartet werden kann.
Keywords: Conservative; Correction limits; Pediatric traumatology section; Retrograde ESIN; Treatment regimen.
© 2024. The Author(s).
Figures




Similar articles
-
[Clavicle shaft fractures in childhood and adolescence : Consensus report of the Pediatric Traumatology Section of the German Society for Trauma Surgery].Unfallchirurgie (Heidelb). 2023 Mar;126(3):244-251. doi: 10.1007/s00113-022-01275-9. Epub 2022 Dec 28. Unfallchirurgie (Heidelb). 2023. PMID: 36576537 German.
-
Proximal humeral fractures in children - controversies in decision making.Eur J Trauma Emerg Surg. 2024 Aug;50(4):1831-1837. doi: 10.1007/s00068-024-02534-7. Epub 2024 Apr 30. Eur J Trauma Emerg Surg. 2024. PMID: 38689019 Free PMC article.
-
[Intraoperative imaging of children and adolescents, for selected fractures and in follow-up after conservative and operative treatment : Part 2 of the results of a nationwide online survey of the Pediatric Traumatology Section of the German Trauma Society].Unfallchirurgie (Heidelb). 2023 Jan;126(1):42-54. doi: 10.1007/s00113-021-01114-3. Epub 2021 Dec 16. Unfallchirurgie (Heidelb). 2023. PMID: 34918188 Free PMC article. German.
-
[Fractures of the upper limbs in childhood and adolescence].Chirurg. 2017 May;88(5):451-466. doi: 10.1007/s00104-017-0420-5. Chirurg. 2017. PMID: 28409214 Review. German.
-
[Shaft fractures in children and adolescents: age-appropriate treatment strategies].Unfallchirurgie (Heidelb). 2025 Jun 13. doi: 10.1007/s00113-025-01594-7. Online ahead of print. Unfallchirurgie (Heidelb). 2025. PMID: 40512399 Review. German.
Cited by
-
[Different expectations regarding the prehospital care of injured children? : A comparison between pediatric surgeons and trauma surgeons].Chirurgie (Heidelb). 2025 Jul 11. doi: 10.1007/s00104-025-02352-6. Online ahead of print. Chirurgie (Heidelb). 2025. PMID: 40643686 German.
References
-
- Ackermann O, Hax P-M, Lahner M, et al. Indikationen zur sonographischen Frakturdiagnostik von Frakturen im Wachstumsalter. Trauma Berufskrankh. 2015;2:115–122. doi: 10.1007/s10039-015-0024-6. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials