

Early trajectories of virological and immunological biomarkers and clinical outcomes in patients admitted to hospital for COVID-19: an international, prospective cohort study
- PMID: 38815595
- PMCID: PMC11181148
- DOI: 10.1016/S2666-5247(24)00015-6
Early trajectories of virological and immunological biomarkers and clinical outcomes in patients admitted to hospital for COVID-19: an international, prospective cohort study
Abstract
Background: Serial measurement of virological and immunological biomarkers in patients admitted to hospital with COVID-19 can give valuable insight into the pathogenic roles of viral replication and immune dysregulation. We aimed to characterise biomarker trajectories and their associations with clinical outcomes.
Methods: In this international, prospective cohort study, patients admitted to hospital with COVID-19 and enrolled in the Therapeutics for Inpatients with COVID-19 platform trial within the Accelerating COVID-19 Therapeutic Interventions and Vaccines programme between Aug 5, 2020 and Sept 30, 2021 were included. Participants were included from 108 sites in Denmark, Greece, Poland, Singapore, Spain, Switzerland, Uganda, the UK, and the USA, and randomised to placebo or one of four neutralising monoclonal antibodies: bamlanivimab (Aug 5 to Oct 13, 2020), sotrovimab (Dec 16, 2020, to March 1, 2021), amubarvimab-romlusevimab (Dec 16, 2020, to March 1, 2021), and tixagevimab-cilgavimab (Feb 10 to Sept 30, 2021). This trial included an analysis of 2149 participants with plasma nucleocapsid antigen, anti-nucleocapsid antibody, C-reactive protein (CRP), IL-6, and D-dimer measured at baseline and day 1, day 3, and day 5 of enrolment. Day-90 follow-up status was available for 1790 participants. Biomarker trajectories were evaluated for associations with baseline characteristics, a 7-day pulmonary ordinal outcome, 90-day mortality, and 90-day rate of sustained recovery.
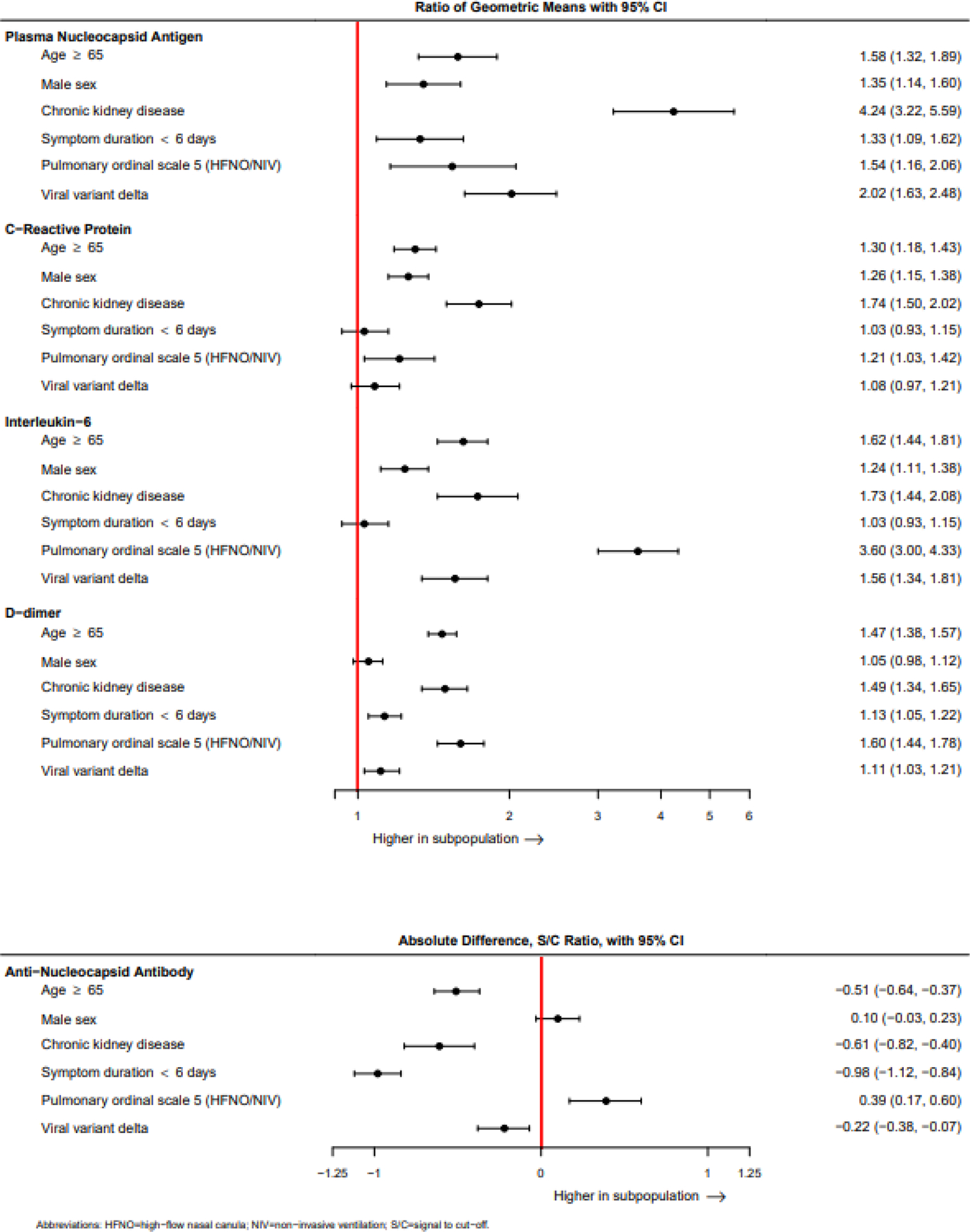
Findings: The study included 2149 participants. Participant median age was 57 years (IQR 46-68), 1246 (58·0%) of 2149 participants were male and 903 (42·0%) were female; 1792 (83·4%) had at least one comorbidity, and 1764 (82·1%) were unvaccinated. Mortality to day 90 was 172 (8·0%) of 2149 and 189 (8·8%) participants had sustained recovery. A pattern of less favourable trajectories of low anti-nucleocapsid antibody, high plasma nucleocapsid antigen, and high inflammatory markers over the first 5 days was observed for high-risk baseline clinical characteristics or factors related to SARS-CoV-2 infection. For example, participants with chronic kidney disease demonstrated plasma nucleocapsid antigen 424% higher (95% CI 319-559), CRP 174% higher (150-202), IL-6 173% higher (144-208), D-dimer 149% higher (134-165), and anti-nucleocapsid antibody 39% lower (60-18) to day 5 than those without chronic kidney disease. Participants in the highest quartile for plasma nucleocapsid antigen, CRP, and IL-6 at baseline and day 5 had worse clinical outcomes, including 90-day all-cause mortality (plasma nucleocapsid antigen hazard ratio (HR) 4·50 (95% CI 3·29-6·15), CRP HR 3·37 (2·30-4·94), and IL-6 HR 5·67 (4·12-7·80). This risk persisted for plasma nucleocapsid antigen and CRP after adjustment for baseline biomarker values and other baseline factors.
Interpretation: Patients admitted to hospital with less favourable 5-day biomarker trajectories had worse prognosis, suggesting that persistent viral burden might drive inflammation in the pathogenesis of COVID-19, identifying patients that might benefit from escalation of antiviral or anti-inflammatory treatment.
Funding: US National Institutes of Health.
Copyright © 2024 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests ALG reports receiving institutional funding from Novavax, institutional partnership with AstraZeneca, and being personally named as inventor on a patent used by AstraZeneca. DDM reports receiving grants from the Danish National Research Foundation. DL reports participation in a study funded by Gilead with no salary support. EM reports payments to his institution received from SciClone Pharmaceuticals, Regeneron Pharmaceuticals, Pfizer, Chemic Labs and KODA Therapeutics, and Cidara, and payment for participating in an advisory board for Basilea. KW reports honorarium for Acute Respiratory Distress Syndrome (ARDS) International Conference in 2023, and travel support from University of California San Francisco. MAM reports institutional funding by the US Department of Defence, Roche-Genetech, and Quantum Health, and personal consulting fees from Gilead, Novartis, and Johnson & Johnson. MKJ reports grants received from Regeneron, Laurent, and Gilead, honoraria from Gilead, and a leadership role with the HIV Medicine Association Board of Directors. PC reports consulting fees from Eli Lilly and Regeneron. All other authors declare no competing interests. All authors were not precluded from accessing data in the study.
Figures



References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
