

Correlation between imaging and histology in benign solitary retroperitoneal nerve sheath tumors: a pictorial review
- PMID: 38816511
- PMCID: PMC11139841
- DOI: 10.1186/s13244-024-01709-5
Correlation between imaging and histology in benign solitary retroperitoneal nerve sheath tumors: a pictorial review
Abstract
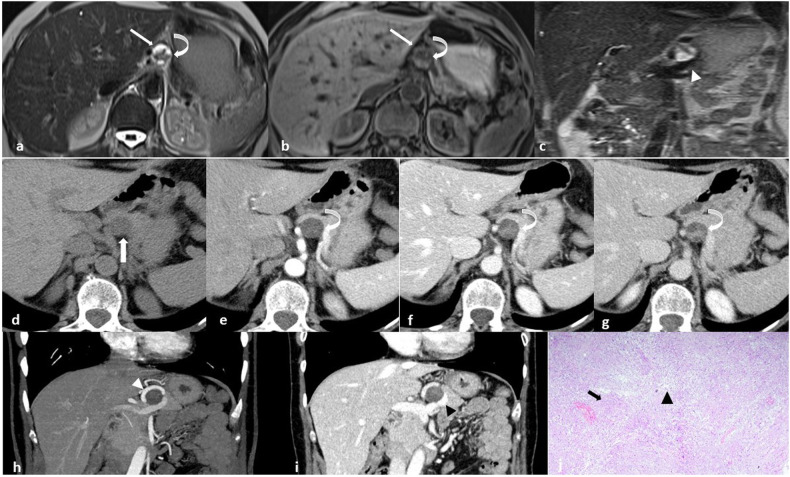
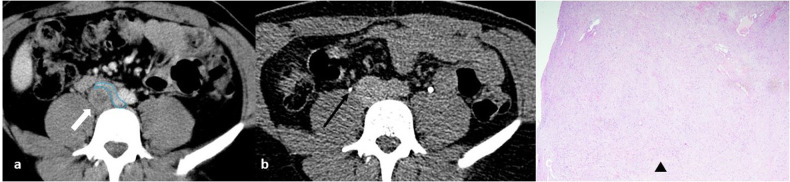
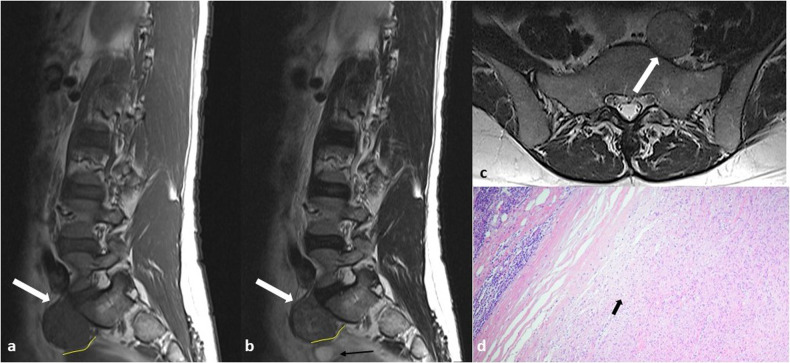
Background: Benign nerve sheath tumors presenting as solitary retroperitoneal masses (RBNSTs) pose a complex diagnostic challenge for multidisciplinary teams regarding differential diagnosis, staging, and treatment planning. This article reviews the role played by different imaging techniques in assessing RBNSTs and elucidates their typical pathological features with a particular emphasis on the correlation between imaging and histological findings. Furthermore, some examples of retroperitoneal tumors that merit consideration in the process of differential diagnosis based on cross-sectional investigations (CSIs) are reported. The correlation between tissue architecture and appearance on imaging can help increase the accuracy of differential diagnosis with other retroperitoneal neoplasms at CSIs.
Critical relevance statement: This educational review critically examines the correlation between imaging and histological features in solitary retroperitoneal benign nerve sheath tumors, offering valuable insights for improving the accuracy of differential diagnosis in clinical radiology.
Key points: RBNSTs are challenging to diagnose because they lack specific radiological features. Differential diagnosis of RBNSTs from other retroperitoneal neoplasms on imaging is complex. Surgical removal of RBNSTs is recommended for an accurate diagnosis.
Keywords: Magnetic resonance imaging; Multidetector computed tomography; Neurofibroma; Retroperitoneal neoplasms; Schwannoma.
© 2024. The Author(s).
Conflict of interest statement
LP is a member of the Scientific Editorial Board for
Figures







References
Publication types
LinkOut - more resources
Full Text Sources
